
You are currently browsing the category archive for the ‘Psychology’ category.
A divorce lawyer is a relationship mechanic.
Wedding planners see shiny new cars. Divorce lawyers see the breakdowns—where things start to strain, where small ignored problems become system failures, where “it happened so suddenly” is almost never true.
In a recent conversation, divorce lawyer James Sexton (25+ years in the trenches) kept returning to one blunt idea:
Most marriages don’t end in a single explosion. They end by dehydration.
People stop paying attention. They stop doing what made their partner feel seen. Resentment piles up quietly. Then one day it looks “sudden,” but it wasn’t. It was slow… then all at once.
So the goal isn’t grand romance. It’s maintenance. And maintenance is unsexy—right up until it saves you.
Here are ten lessons worth stealing.
1) Pay attention like it’s alive
The fastest route to divorce isn’t one dramatic betrayal. It’s the belief that “we’re married now, so we’re good.”
Marriage isn’t a trophy you put on a shelf. It’s a living thing. If you stop tending it, it doesn’t stay “fine.” It withers.
Try this: do one small “I see you” action every day—thank you, a compliment, a quick note, a small touch, a check-in.
2) Keep doing the “dating behaviors”
Early on, you pursued. You were curious. You made effort. You were interested—and interesting.
Then life arrives: work, kids, exhaustion, routines. Couples treat courtship like a one-time entrance fee instead of the ongoing engine of closeness.
The boring truth is also the saving truth:
the behaviors that “won” your partner are the behaviors that keep your partner.
Try this: once a week, do something you would’ve done when you were trying to impress them—plan something, initiate, make it clear they’re still chosen.
3) Break the spiral before it becomes your normal
A lot of unhappy marriages get stuck in loops that feel logical from the inside:
- “You don’t want me.”
- “I don’t want you because you don’t seem to like me.”
- “I don’t seem to like you because we’re never close.”
- “We’re never close because life is chaos.”
Eventually you land in the worst place: both people feel justified, and both feel lonely.
The key insight: spirals can be reversed with the same simplicity that created them.
Not by “winning” an argument, but by shifting the emotional direction.
Try this: be the first person to do the generous thing—kindness, help, warmth—before you feel like you’ve “earned” it.
4) Talk when it’s smoke, not fire (“hit send now”)
A common divorce pattern is small grievances saved up until they become ammunition. Then one day you’re fighting about something ridiculous… and suddenly it’s about ten years of unresolved hurt.
Sexton’s advice is to speak early—before the issue becomes a story you tell yourself.
It doesn’t have to be a confrontation. It can be a calm check-in.
Try this:
“Small thing: when you said X, it sat weird with me. I might be misreading it, but I wanted to check.”
5) Frame complaints as longing, not prosecution
The same concern can either invite closeness or trigger defense.
- “We never have sex.”
vs - “I miss feeling close to you.”
One is a charge sheet. The other is a bid for connection.
People can fight accusations. It’s harder to fight honest longing.
Try this: translate “you never” into “I miss…” and “I want…”
6) Praise isn’t fluff—it’s preventative medicine
Many people treat compliments as optional. Then they wonder why warmth dries up.
Appreciation is not a “nice extra.” It’s lubrication for the whole machine. It’s how you stay emotionally fed in the middle of real life.
Try this: one specific compliment per day. Not “you’re great,” but:
“I loved how you handled that.”
“You looked amazing today.”
“I felt proud standing beside you.”
7) Treat money secrecy as a real betrayal
Sexton emphasizes that “financial betrayal” ends a lot of marriages: hidden debt, secret spending, stability that turns out to be a house of cards.
It’s not the dollars that destroy trust. It’s the deception—the feeling that you were not a teammate.
Try this: make money boring and routine: a monthly check-in on spending, debts, goals, and anxieties. No drama. Just truth.
8) Expect stress gates—and navigate them together
Relationships strain at predictable transition points:
- a new baby
- kids becoming less dependent
- career shifts
- bodies aging
- midlife “is this it?” questions
- empty nest
The failure mode is drift: two people building separate lives under one roof.
Try this: name the transition out loud:
“We’re entering a new phase. How do we protect us inside it?”
9) Social media can quietly poison gratitude
Sexton’s line is memorable: social media is often “everyone’s greatest hits while you live your gag reel.”
If you scroll passively, you absorb the message that everyone else’s life is easier, sexier, more exciting—and that your relationship is uniquely flawed.
This isn’t moral panic. It’s attention economics: what you stare at trains your desires and your dissatisfaction.
Try this: curate aggressively. Feed the content that strengthens your bond. Starve the content that erodes it. If you can’t do that, limit the exposure.
10) The hard thing and the right thing are usually the same
When people drift toward cheating or quitting, the clean move is not secrecy. It’s honesty while there’s still time.
Something like:
“We’re far apart. I’m lonely. I’m tempted. Can we fix this—together?”
That conversation is terrifying. It is also the one that keeps your integrity intact—and often saves the marriage before it crosses lines you can’t uncross.
Try this: don’t romanticize “the drift.” Name it early.
A simple weekly ritual (10 minutes)
If you want one habit instead of ten ideas, steal this:
- One appreciation: “This week I felt loved when you…”
- One repair: “This week I felt a sting when…”
- One desire: “This week I’d love more…”
- One plan: “This week, let’s protect time for us on…”
Short. Regular. Honest.

The quiet thesis
Most marriages don’t die from one villainous act. They die from inattention + unspoken resentment + unmanaged transition—and then, eventually, the predictable betrayals that follow disconnection.
The fix is not constant fireworks.
It’s steady proof—small, consistent proof—that your partner is still chosen.
Water the plant. Before it looks dead.
Canada’s Bill C-4 was sold as a targeted ban on abusive “conversion therapy.” That goal of ending coercive, shame-based attempts to “pray the gay away”is legitimate, and the harms from such practices are well documented. (Library of Parliament)
But C-4 didn’t stop at prohibiting coercion. It built contested premises about “gender identity” into the Criminal Code—then wrapped ordinary clinical caution in legal risk. For children, that’s not a symbolic problem. It’s a downstream harm problem.
1) C-4 hard-codes a contested concept into criminal scope
The Criminal Code definition of “conversion therapy” includes any “practice, treatment or service designed to… change a person’s gender identity to cisgender,” or “repress… a person’s non-cisgender gender identity.” (Department of Justice Canada)
That’s not the same category as sexual orientation. Whatever one’s politics, “gender identity” is not measured like blood pressure. In real child psychotherapy, you do differential diagnosis: you test hypotheses, you treat comorbidities, you watch patterns over time, you revisit interpretations.
C-4 makes one interpretive direction toward “cisgender”a uniquely danger to be seen as the “design” of therapy. (Department of Justice Canada)
2) The preamble signals something stronger than “don’t abuse people”
The Act’s preamble denounces “myths and stereotypes,” including “the myth that… cisgender gender identity… [and] gender expression that conforms to the sex assigned… are to be preferred over other… gender identities.” (Parliament of Canada)
Supporters will say this is a dignity claim: no one should be pressured to “be cis.” Fine. But when Parliament declares a core premise a “myth,” it doesn’t just condemn abuse it pressures institutions to treat skepticism as suspect.
In therapy, that matters, because the clinician’s job is not to recite a moral slogan. It’s to find the causal engine of distress in a specific child.
3) “Exploration” is permitted—until it looks like exploration with a destination
C-4 includes a “for greater certainty” carve-out for “exploration or development of an integrated personal identity… such as… gender transition,” provided the service is not “based on an assumption that a particular… gender identity… is to be preferred over another.” (Department of Justice Canada)
Here’s the problem: in actual clinical practice, the line between exploration and influence is not a clean statutory boundary.
A careful therapist might say:
- “Let’s treat anxiety/OCD first and see what remains.”
- “Let’s explore trauma and dissociation before we interpret identity claims.”
- “Let’s reduce online reinforcement and stabilize sleep, mood, and social stress.”
- “Let’s slow down—puberty is a confounder, not an oracle.”
That’s not “conversion.” That’s normal clinical sequencing.
But under C-4’s language, a motivated complainant (or risk-averse administrator) can reframe caution as an attempt to “repress” a non-cis identity, or as therapy “designed” to steer toward “cisgender.” (Department of Justice Canada)
Even if a prosecution is unlikely, the chilling effect doesn’t require convictions. It only requires enough ambiguity that clinicians and clinics decide it’s not worth the exposure.
4) This isn’t “college policy.” It’s Criminal Code territory.
Bill C-4 received Royal Assent on December 8, 2021 and came into force in January 2022. (Parliament of Canada)
It created Criminal Code offences around causing someone to undergo conversion therapy, promoting/advertising it, and profiting from it. (Parliament of Canada)
So when therapists ask, “Can I safely do exploratory work with this child without being accused of ‘conversion’?” they are not being melodramatic. They are doing what professionals do when lawmakers write broad definitions: they assume the worst plausible reading—and they self-censor.
5) Why this hits children hardest
Adults can absorb bad ideology and still have time to course-correct. Kids often can’t.
Children need therapy that is:
- exploratory (many hypotheses, not one script),
- developmentally sober (puberty changes the picture),
- comorbidity-first (anxiety, depression, autism traits, trauma, dissociation),
- family-systems aware (parents are usually the safety net, not “the enemy”),
- outcome-humble (no foreclosed conclusions).
C-4 subtly tilts the playing field: it makes “don’t be seen as steering away from trans identity” the safest institutional posture regardless of whether that posture serves the child in front of you.
6) Why this question is sharper now
After the February 10, 2026 Tumbler Ridge shootings, public attention has turned—again—to institutional failure chains: mental health, gatekeeping, warning signs, and what “care” actually means when a young person is unstable. The BC RCMP’s Feb 13 update refers to autopsies for “eight victims and the suspect” (nine deceased total), and notes ongoing review of prior interactions with the suspect. (RCMP)
A tragedy doesn’t “prove” a policy critique. But it does remove the luxury of pretending that scripts are the same thing as safeguards.
A better standard (without reviving abusive conversion practices)
If Parliament’s aim is to ban coercion and fraud, it can do so cleanly without criminalizing clinical caution.
A fix would explicitly protect:
- Open-ended psychotherapy for gender distress, including differential diagnosis and comorbidity treatment.
- Neutral therapeutic goals (reducing distress, improving functioning, strengthening self-acceptance) without predetermining identity outcomes.
- The clinician’s ability to discuss biological sex reality, uncertainty, and developmental pathways without that being treated as “preference” or “myth.” (Parliament of Canada)
- Bright-line prohibitions aimed at the actual evils: coercion, aversive techniques, confinement, threats, and misrepresentation.
Canada can still denounce abuse and defend evidence-based exploration. Kids deserve therapists unbound by ideology—not just ideology unbound by evidence.

References
- Bill C-4 — First Reading (House of Commons) — Nov 29, 2021
https://www.parl.ca/DocumentViewer/en/44-1/bill/C-4/first-reading
Source: (Parliament of Canada) - Bill C-4 — Third Reading (House of Commons) — Dec 1, 2021
https://www.parl.ca/DocumentViewer/en/44-1/bill/C-4/third-reading
Source: (Parliament of Canada) - Bill C-4 — Royal Assent (Chapter 24) — Dec 8, 2021
https://www.parl.ca/DocumentViewer/en/44-1/bill/C-4/royal-assent
Source: (Parliament of Canada)
Core legal text (Criminal Code, consolidated)
- Criminal Code — s. 320.101 (definition + exploration carve-out)
https://laws-lois.justice.gc.ca/eng/acts/c-46/section-320.101.html - Statutes of Canada 2021, c. 24 (Annual Statutes full text — includes preamble)
https://laws-lois.justice.gc.ca/eng/AnnualStatutes/2021_24/FullText.html
Official legislative record / metadata (timeline, status)
- LEGISinfo — Bill C-4 (44-1) (dates, stages, summary trail)
https://www.parl.ca/legisinfo/en/bill/44-1/c-4
Source: (Parliament of Canada)
Neutral institutional summary
- Library of Parliament — Legislative Summary (PDF)
https://publications.gc.ca/collections/collection_2022/bdp-lop/ls/YM32-3-441-C4-eng.pdf
Source: (Government of Canada Publications)
Government explainer / enforcement framing
- Justice Canada — “Conversion therapy” page (in-force date, offences overview)
https://www.justice.gc.ca/eng/rp-pr/jr/ct-tc/p1.html
Context reference used in the essay (Tumbler Ridge)
- RCMP — Tumbler Ridge investigative update (Feb 13, 2026)
https://rcmp.ca/en/bc/tumbler-ridge/news/2026/02/4350292
Modern psychology has a recurring weakness. It periodically falls in love with stories that feel morally urgent, then struggles to unwind them when the evidence turns out thin. That is not because psychologists are uniquely foolish. It is because the field studies messy human beings with noisy measures, ambiguous constructs, and strong social incentives. In that environment, a persuasive narrative can get promoted into “settled science” long before it is actually settled.
The replication crisis is the clearest public sign of this vulnerability. The Reproducibility Project’s large collaboration tried to replicate 100 psychology studies and found much weaker effects and far fewer statistically significant replications than the original literature suggested. (Science) Methodologists also showed how flexible analysis choices and reporting can inflate false positives unless stricter norms are enforced. (SAGE Journals) Meehl’s older critique still lands for the same reason: in “soft” areas of psychology, theories often fade away rather than being cleanly tested and retired. (Error Statistics Philosophy) The implication is not nihilism. It is epistemic humility, especially for claims that are politically charged and personally consequential.
Psychology’s history offers examples of ideas that persist on social momentum long after the evidence grows cloudy. The “memory wars” around repressed and recovered memories show how a compelling clinical narrative can endure in practice while mechanisms remain disputed, and how suggestion can complicate confident storytelling. (PMC) Lilienfeld and colleagues made the broader point in a different domain: weak measurement, loose constructs, and credulous clinical fashions predict confident claims that later demand painful correction. (Guilford Press) The pattern is simple: psychology is unusually prone to ideas becoming socially protected before they are empirically solid.
That is the right context for the strong activist version of “innate gender identity,” meaning the claim that very young children can reliably know and articulate a fixed inner gender that may mismatch their body, and that this knowledge should be treated as stable guidance for major decisions. Developmentally, this is exactly the kind of adult projection Piaget and Erikson warn against: treating children’s words as if they carry stable adult concepts while the child’s understanding and self-organization remain socially shaped and changeable. Even within clinical samples, trajectories are not uniform; intensity of childhood gender dysphoria is one known factor associated with persistence into adolescence, which is another way of saying early self-labels do not function like a universal diagnostic oracle. (PubMed) Clinically, the major classification systems are more cautious than the slogans: DSM-5-TR defines gender dysphoria around clinically significant distress or impairment, not the mere existence of an identity claim. (American Psychiatric Association) ICD-11 moved gender incongruence out of the mental disorders chapter and into “conditions related to sexual health,” partly to reduce stigma while preserving access to care. (World Health Organization)
The evidence environment around youth gender medicine shows why fad dynamics matter. The Cass Review argued the evidence base for medical interventions in minors is limited and often low certainty, urging caution and better research. (Utah Legislature) Substantial critiques dispute Cass’s methods and interpretation, which itself signals this is not a stable, high-consensus evidentiary domain. (PMC) The adult responsibility is therefore straightforward: treat childhood self-labels as developmentally real but conceptually limited; separate distress from metaphysics; demand the same evidentiary standards you would demand anywhere else in medicine; and resist turning a contested construct into a moral absolute. If psychology keeps rewarding certainty over rigor, the cost will not be merely bad theory. It will be policy and clinical practice that harden too early, then harm real people when the correction finally arrives.

Glossary
- Replication / reproducibility: Whether an independent team can rerun a study and obtain broadly similar results. (Science)
- Researcher degrees of freedom: The many choices researchers can make (when to stop collecting data, which outcomes to report, which analyses to run) that can unintentionally inflate “significant” findings. (SAGE Journals)
- P-hacking: Informal term for exploiting analytic flexibility to chase statistical significance. (SAGE Journals)
- Construct validity: Whether a measure actually captures the concept it claims to measure (not just something correlated with it). (General measurement concern emphasized in clinical-science critiques.) (Guilford Press)
- Gender dysphoria (DSM-5-TR): Clinically significant distress or impairment related to gender incongruence; not all gender-diverse people have dysphoria. (American Psychiatric Association)
- Gender incongruence (ICD-11): ICD-11 category placed under “conditions related to sexual health,” moved out of the mental disorders chapter. (World Health Organization)
- Persistence (in childhood GD research): Continued gender dysphoria into adolescence; research suggests persistence is not uniform, and intensity is one associated factor. (PubMed)
Short endnotes (audit-friendly)
- Replication crisis anchor: Open Science Collaboration (2015), Science; effects in replications notably smaller; fewer significant replications. (Science)
- Analytic flexibility / false positives: Simmons, Nelson & Simonsohn (2011), “False-Positive Psychology.” (SAGE Journals)
- Soft-psychology theory fade-out critique: Meehl (1978), “Theoretical Risks and Tabular Asterisks: Sir Karl, Sir Ronald, and the Slow Progress of Soft Psychology.” (Error Statistics Philosophy)
- Memory wars as an example of contested clinical narratives: Otgaar et al. (2019, PMC) on repression controversy; Loftus (2006) review on recovered/false memories; Loftus (2004) in The Lancet on the continuing dispute. (PMC)
- Clinical-science warning about fads/pseudoscience: Lilienfeld et al., Science and Pseudoscience in Clinical Psychology (Guilford excerpts / volume). (Guilford Press)
- DSM-5-TR framing: APA overview and DSM-related materials emphasize distress/impairment as the diagnostic core. (American Psychiatric Association)
- ICD-11 move and rationale: WHO FAQ; supporting scholarly rationale for moving gender incongruence out of mental disorders while preserving access to care. (World Health Organization)
- Persistence factor (intensity): Steensma et al. (2013) follow-up: intensity of childhood GD associated with persistence. (PubMed)
- Cass Review debate: Cass Review final report PDF (archived copies); published critiques and responses indicating contested interpretation and ongoing debate. (Utah Legislature)
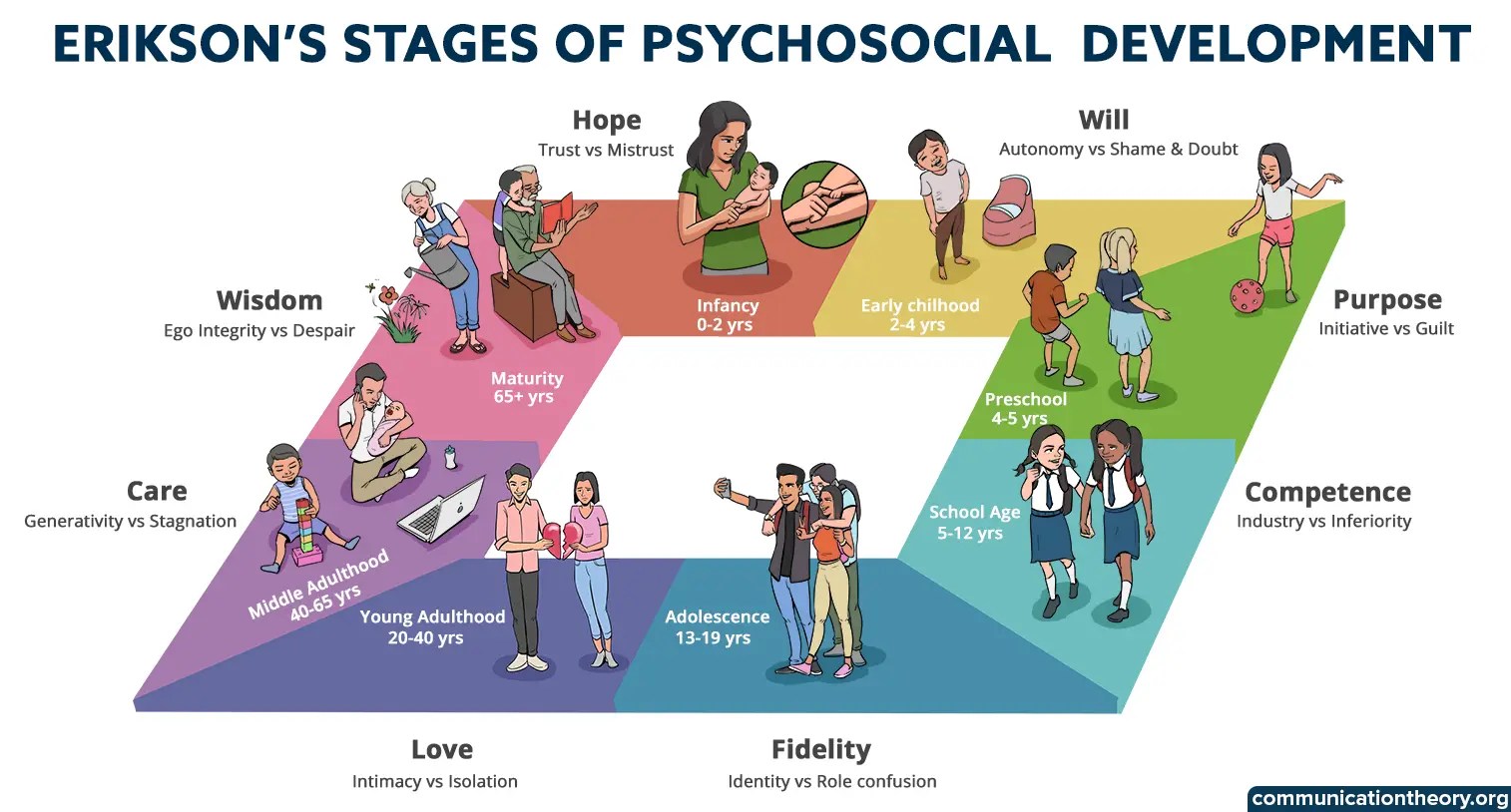
Erik Erikson is still useful because he blocks a modern temptation: reading a child’s self-descriptions as evidence of a finished, stable identity. For Erikson, identity is not an inner essence that appears early and then merely announces itself. It is something built across time under social conditions. Relationships, cultural scripts, permissions, limits, and feedback all shape what a person can plausibly become and what they can sustain. If you want a single takeaway, it is this: adults regularly project mature coherence onto children whose sense of “who I am” is still under construction. (The Psychology Notes Headquarters)
Erikson’s framework is psychosocial. He describes eight broad stages across the lifespan, each organized around a tension between two outcomes. The point is not a one-time pass or fail. It is a developmental task that tends to recur in new forms as life changes. When conditions are supportive, people lean toward the positive resolution and develop an associated strength or “virtue.” When conditions are hostile or mismatched, the negative pole can dominate and leave a durable vulnerability. (The Psychology Notes Headquarters)
In early childhood, the tasks are basic but not trivial. In infancy, trust versus mistrust is shaped by whether care is reliable and responsive. In toddlerhood, autonomy versus shame and doubt turns on whether a child can attempt self-control without being humiliated for mistakes. In the preschool years, initiative versus guilt turns on whether exploration and planning are welcomed or punished. These are not destiny. They are early patterns. They set default expectations about safety, agency, and permission that can be reinforced later or revised by later experience. (The Psychology Notes Headquarters)
School age brings industry versus inferiority. Children now meet the world of tasks, standards, and comparison. Competence grows when effort produces mastery and feedback is fair. Inferiority grows when failure is repeated, demands are mismatched, or judgment is harsh. This matters because it supplies the raw materials for adolescence. Identity versus role confusion is not about picking a label. It is about synthesizing roles, values, loyalties, and a changing body into something that feels continuous and workable. Researchers made this more testable by focusing on processes like exploration and commitment (roughly, trying roles out and then making durable choices), yielding familiar identity-status patterns such as diffusion, foreclosure, moratorium, and achievement. Longitudinal work also supports the commonsense point that identity development extends beyond the teen years for many people. (The Psychology Notes Headquarters)
Erikson’s model deserves the criticisms it often receives. The stages function best as descriptive heuristics rather than strict schedules, and some concepts are hard to measure cleanly. The framework also reflects mid-20th-century Western assumptions, and feminist scholarship has pressed on its gendered blind spots. Still, the core insight survives: selfhood is social before it is philosophical. Children become “someone” through attachment, modeling, constraint, opportunity, and recognition. The practical reminder is blunt, feeding directly into today’s debates. Do not read adult-level identity stability into young children’s words or preferences. Much of what looks like certainty in a child is a snapshot of roles and reinforcement, not proof of a permanent inner core. (The Psychology Notes Headquarters)
Glossary
- Psychosocial stage/task: A recurring developmental challenge shaped by social context, not a biological timer. (The Psychology Notes Headquarters)
- Virtue (Erikson): A strength associated with a relatively positive resolution of a stage task (e.g., hope, will, competence, fidelity). (The Psychology Notes Headquarters)
- Identity vs role confusion: The adolescent task of developing a workable sense of continuity across roles, values, and future direction. (The Psychology Notes Headquarters)
- Identity statuses (Marcia tradition): A research approach using exploration and commitment to classify patterns like diffusion (low both), foreclosure (commitment without exploration), moratorium (exploration without commitment), and achievement (exploration leading to commitment). (Wikipedia)
Endnotes
- Erikson stages overview, virtues, and the “not pass/fail” framing: StatPearls (Orenstein, 2022). (The Psychology Notes Headquarters)
- Scholarly overview and modern framing of Erikson as a lifespan theory: Syed & McLean (2017, PsyArXiv).
- Identity-status trajectories and measurement of exploration/commitment over time: Meeus (2011, PMC). (Wikipedia)
- Marcia identity-status grounding in Eriksonian identity crisis: foundational identity-status paper (PDF record).
- Feminist critique and gender-bias discussion of Eriksonian identity: Sorell (2001).
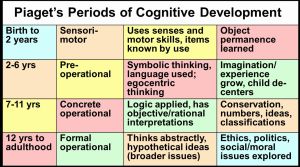
Jean Piaget is still worth reading because he blocks a common adult mistake: treating children’s words as if they carry adult concepts. Children do not merely know fewer facts. They use different cognitive tools at different ages, and those tools change what their categories can mean. That matters whenever adults take a child’s self-label and translate it into a fixed inner essence. Piaget’s basic warning is simple: the same vocabulary can sit on top of a different kind of understanding, and adults are very good at smuggling their own meanings into what a child says. The rest of his theory is an attempt to explain why that translation error is so easy to make.
Piaget’s machinery for explaining the gap is spare and still useful. Children build schemas, mental frameworks for understanding objects, actions, and categories. They update those schemas through assimilation, which fits new experience into an existing framework, and accommodation, which changes the framework when the fit fails. The friction between “make it fit” and “change the model” is not a bug. It is the engine. Piaget calls the longer-term settling of that friction equilibration, the push toward a workable balance where the child’s model of the world holds together and predicts better.
Piaget is best known for his four-stage outline. In the sensorimotor stage (birth to about 2), infants learn through perception and action, and one classic milestone is object permanence, the idea that things still exist when out of sight. In the preoperational stage (about 2 to 7), children gain symbolic thought: language, pretend play, mental imagery. They also show characteristic limits on many tasks, including egocentrism in perspective-taking and failures of conservation (for example, thinking a taller glass has “more” of the same liquid).
Those limits are real, but they are not always as simple as “the child cannot do it.” Modern researchers have shown that the timing can shift when you change the method. Studies using “violation-of-expectation” designs often find signs of earlier object knowledge than Piaget’s original search tasks detected. The clean takeaway is not that Piaget collapses. It is that measurement matters. Some tasks load children with extra demands (motor planning, inhibition, working memory) that can hide understanding that is present in a simpler form. Task demands can mask competence.
In the concrete operational stage (about 7 to 11), children become capable of logical operations tied to tangible situations. Conservation stabilizes, classification becomes more systematic, and seriation appears more reliably, as when a child can order sticks from shortest to tallest without guesswork. In formal operational thought (roughly adolescence onward, and unevenly across people and domains), abstract and hypothetical reasoning becomes more consistent. Even here, performance can be uneven across closely related tasks, a pattern discussed under the label horizontal décalage. That unevenness is a warning against treating stages as rigid ceilings. Read them instead as a map of typical reorganizations in thinking: a useful guide to what changes, and when, without pretending every child hits every milestone on the same schedule. The practical payoff is blunt. When adults treat a child’s words as adult-level commitments, they risk importing meanings the child has not yet built.
Glossary
- Schema: A mental framework for organizing and interpreting experience.
- Assimilation: Fitting new experience into an existing schema.
- Accommodation: Modifying a schema when the old one does not fit.
- Equilibration: The balancing process that restores or maintains cognitive stability through assimilation and accommodation.
- Object permanence: Understanding that objects continue to exist when hidden.
- Conservation: Understanding that quantity stays the same despite changes in appearance if nothing is added or removed.
- Horizontal décalage: Uneven mastery across related tasks; competence does not arrive all at once.
Endnotes
- Encyclopedia Britannica — Piaget overview: stages, age ranges, and constructivist framing.
- APA Dictionary of Psychology — Piagetian terms: schema, assimilation, accommodation.
- APA Dictionary of Psychology — “Equilibration” definition.
- Baillargeon, Spelke & Wasserman (1985) — early object knowledge via violation-of-expectation methods (PubMed record and related materials).
- Lourenço (2016) — stages as conceptual tools/heuristics (ScienceDirect).
- Neo-Piagetian review discussing horizontal décalage and unevenness as a complication for strict stage-uniformity (UCL Press journals).
In late December 2025, an X thread went viral by naming a pattern many people recognize but rarely formalize. The author argued that much contemporary activism doesn’t begin with an argument. It begins with an emotional capture: a suffering child, a traumatized testimonial, a stripped-down historical grievance, a demand to “listen,” and the implicit message that hesitation is moral failure. If the target asks for definitions, tradeoffs, or evidence, the thread claims the response is often not rebuttal but stigma—labels meant to raise the social cost of dissent.
To describe the mechanism, the thread borrows from psychologist Martha Stout’s The Sociopath Next Door, especially her warning about the “pity play”: an appeal to sympathy that disarms decent people and grants the manipulator moral cover. The point of the thread is not that political opponents are “sociopaths.” Its point is that sympathy can be used to purchase moral immunity, and once immunity is granted, scrutiny becomes taboo.
This matters because democratic persuasion depends on the difference between compassion and coercion. Compassion is attention to suffering. Coercion is using suffering to forbid questions.
So here is a practical test for readers who want to stay humane without becoming steerable.
The Narrative Pressure Test
When a cause arrives wrapped in urgency, run five questions before you assent.
1) What claim is being made, separate from the story?
A vivid story is not a thesis. A photo is not a policy. If the emotional payload is clear but the claim is vague, you’re being recruited before you’re informed.
A common trick is to start with something true (“this person is suffering”) and slide toward something contestable (“therefore this specific policy is the only decent response”). The bridge between those two is where reasoning belongs. If the bridge is missing, the message is operating as a shortcut.
2) What facts would falsify it?
Real claims have losing conditions. If disagreement itself is treated as evidence of malice, the message isn’t trying to persuade. It’s trying to sort people into “good” and “bad.”
This is where moral language becomes a weapon. “Act now or you’re complicit” is not analysis. It is time pressure dressed as conscience.
3) Who gets moral immunity?
Look for the doctrine of permanent innocence.
If a group is treated as incapable of agency, it will also be treated as incapable of responsibility. That exemption attracts opportunists and rewards escalation, because any request for standards can be reframed as “attacking victims.”
Pity is not the problem. Pity used as a shield against scrutiny is.
4) What action is being demanded, and who pays?
This question forces morality to meet arithmetic.
Is the demanded action symbolic (slogans, rituals, purges), or coercive (law, policy, firings, spending commitments, policing changes)? Who bears the downside risk? The people demanding sacrifice, or the bystanders who can’t opt out?
If the loudest moralizers don’t pay the costs, compassion may be functioning as status performance rather than responsibility.
5) What happens if we slow down?
True emergencies can survive scrutiny. Manufactured urgency cannot.
If a narrative collapses the moment you ask for definitions, evidence, and tradeoffs, it’s not designed to be tested. It’s designed to capture. The insistence on speed is often the tell, because speed bypasses the hard questions that expose weak claims.
The steelman objection
There is an obvious fear here: doesn’t this “weaponized empathy” framework become an excuse to ignore suffering?
It can. That’s the failure mode in the opposite direction. People learn the language of manipulation and use it as an anesthetic: any appeal to pain becomes “a pity play,” and they never have to do anything difficult again.
The disciplined position is harder:
-
Suffering is real and morally relevant.
-
Claims made on the back of suffering still need scrutiny.
-
Compassion is not permission to skip consequences.
A clean rule helps: grant humanity first, then demand the adult questions.
A person can be hurting and still be wrong. A cause can be sympathetic and still produce harm. A story can be true and still be used to sell a false conclusion.
Compassion with guardrails
The viral thread’s usefulness is not in its tribal conclusions. It is in the reminder that moral pressure can substitute for argument, and that good people are especially vulnerable to that substitution because they don’t want to be cruel.
The antidote is not numbness. It is sequencing. Feel the tug, then force the questions.
Empathy is a virtue. But empathy that cannot tolerate scrutiny becomes a lever. And a society that hands out levers this easily will eventually be moved by whoever learns to pull them best.

References
Ne_pas_couvrir X thread (Dec 23, 2025)
https://x.com/Ne_pas_couvrir/status/2003469502210572613
Martha Stout — “pity play” quote (Goodreads)
https://www.goodreads.com/quotes/1129543-rather-the-best-clue-is-of-all-things-the-pity
Martha Stout — The Sociopath Next Door (Goodreads quotes index)
https://www.goodreads.com/work/quotes/118905-the-sociopath-next-door
Bezmenov context (Snopes)
https://www.snopes.com/fact-check/1960s-kgb-experiments-subjects-brainwashed/
Bezmenov overview (Big Think)
https://bigthink.com/the-present/yuri-bezmenov/
“Trump Derangement Syndrome” (TDS) isn’t a medical condition. It’s a rhetorical label for a recognizable pattern: Donald Trump becomes the organizing centre of political perception, so that every event is interpreted through him, and every interpretation is pulled toward maximal moral heat. Even people who agree on the facts can’t agree on the temperature, because the temperature is the point. Psychology writers describe it as a derogatory term for toxic, disproportionate reactions to Trump’s statements and actions.
And when politicians try to literalize it as a clinical diagnosis, it collapses into farce. It is fundamentally a political phenomenon, not a psychiatric one.
The useful question isn’t “Is Trump uniquely bad?” Reasonable people can say yes on qualities character, norms, rhetoric, policy, whatever. The useful question is: when does valid criticism become TDS? The answer is: when Trump stops being an object of analysis and becomes a gravity well.
What TDS looks like (beyond normal criticism)
Normal criticism is specific: this policy, this consequence, this evidence, this alternative. TDS is different in kind.
-
Totalization: Trump isn’t a president with a platform; he’s a single-cause explanation for everything.
-
Asymmetry: Similar behaviour in other leaders is background noise; in Trump it becomes existential threat (or, on the other side, heroic 4D chess).
-
Incentive blindness: The critic’s emotional reward (“I signaled correctly”) overrides the duty to be precise.
-
Predictable misreads: Even when Trump does something ordinary or mixed, it must be either apocalypse or genius.
This is why the term persists. It points generallyat a real cognitive trap: a personality-driven politics that makes judgment brittle. (It also gets used cynically to dismiss legitimate criticism; that’s part of the ecosystem, too.)
Why Canadian media amplifies it
Canada didn’t invent Trump fixation. But Canadian legacy media has strong reasons to keep Trump on the homepage. The reasons, in question, are not purely ideological.
1) Material proximity (it’s not “foreign news” in Canada).
When the U.S. president threatens tariffs, trade reprisals, or bilateral negotiations, Canadians feel it directly: jobs, prices, investment, and national policy all move. In Trump’s second term, Canadian economic and political life has repeatedly been forced to react to U.S. pressure: tariffs, trade disputes, and negotiations that shape Ottawa’s choices.
That creates a built-in news logic: Trump coverage is “domestic-adjacent,” not optional.
2) An attention model that rewards moral theatre.
Trump is an outrage engine. Outrage is a business model. Canadian mediais operating in a trust-and-revenue squeeze, and that squeeze selects for stories that reliably produce engagement. Commentators on Canada’s media crisis have argued that the Trump era intensified the trust spiral and the incentives toward heightened, adversarial framing.
3) Narrative convenience: Trump as a single, portable explanation.
Complex stories (housing, health systems, provincial-federal dysfunction) are hard. Trump is easy: one villain (or saviour), one emotional script, one endless drip of “breaking.” This is where amplification turns into distortion. A real cross-border policy dispute becomes a morality play; a complicated negotiation becomes a personality drama.
4) Coverage volume becomes self-justifying.
Once a newsroom commits, it has to keep feeding the lane it created. Tools that track Canadian legacy-media coverage of Trump-related economic conflict like tariffs for example, show how sustained and multi-outlet that attention can become.
The more space Trump occupies, the more “newsworthy” he becomes, because “everyone is talking about it” (including the newsroom).
None of this requires a conspiracy. It’s mostly incentive alignment: relevance + engagement + a simple narrative hook.
The cost: Canadians inherit America’s temperature
The predictable result is that Canadians import not just U.S. events, but U.S. emotional calibration.
-
Canadian politics gets interpreted as a shadow-play of American factions.
-
Domestic accountability weakens (“our problems are downstream of Trump / anti-Trump”).
-
Readers get trained to react first and think second, a reinforcing heuristic, because that’s what the coverage rewards.
And it corrodes trust: if audiences can feel when coverage is performing emotional certainty rather than reporting reality, they stop believing the institution is trying to be fair.
A reader’s heuristic: the TDS check
If this is going to be useful (not tribal), it needs a diagnostic you can run on yourself and on coverage:
-
Specificity test: Is the criticism about a policy and its consequences, or about Trump as a symbol?
-
Symmetry test: Would you report/feel the same way if a different president did it?
-
Proportionality test: Does the language match the evidence, or does it leap straight to existential claims?
-
Update test: When new facts arrive, does the story change—or does the narrative stay fixed?
-
Trade-off test: Are costs and alternatives discussed, or is “opposition” treated as sufficient analysis?
Pass those tests and you’re probably doing real criticism. Fail them repeatedly and you’re in the gravity well regardless of whether the content is rage or adoration.
The verdict
Trump is a legitimate target for strong criticism especially in a second term with direct consequences for Canada.
But the deeper media failure is not “being anti-Trump.” It’s outsourcing judgment to a narrative reflex: a system that selects for maximal heat, maximal frequency, and minimal precision. That’s how valid critique curdles into derangement—because it stops being about what happened, and becomes about what the story needs.
The fix is boring, which is why it’s rare: lower the temperature, raise the specificity, and let facts earn the conclusion.

Psychology Today — “The Paradox of ‘Trump Derangement Syndrome’” (Sep 5, 2024)
https://www.psychologytoday.com/ca/blog/the-meaningful-life/202409/the-paradox-of-trump-derangement-syndrome
The Loop (ECPR) — “Is ‘Trump Derangement Syndrome’ a genuine mental illness?” (Oct 13, 2025)
CBS News Minnesota — “Minnesota Senate Republicans’ bill to define ‘Trump derangement syndrome’ as mental illness…” (Mar 17, 2025)
https://www.cbsnews.com/minnesota/news/trump-derangement-syndrome-minnesota-senate-republicans/
Reuters Institute — Digital News Report 2025: Canada (Jun 17, 2025)
https://reutersinstitute.politics.ox.ac.uk/digital-news-report/2025/canada
The Trust Spiral (Tara Henley) — The state of media/trust dynamics (May 2024)
Reuters — “Trump puts 35% tariff on Canada…” (Jul 11, 2025)
https://www.reuters.com/world/us/trump-puts-35-tariff-canada-eyes-15-20-tariffs-others-2025-07-11/
Financial Times — “Canada scraps tech tax to advance trade talks with Donald Trump” (Jun 30, 2025)
https://www.ft.com/content/4cf98ada-7164-415d-95df-43609384a0e2
The Guardian — “White House says Canadian PM ‘caved’ to Trump demand to scrap tech tax” (Jun 30, 2025)
https://www.theguardian.com/world/2025/jun/30/canada-digital-services-tax-technology-giants-us-trade-talks
The Plakhov Group — Trade War: interactive visualizations of Canadian legacy-media coverage of Trump’s tariffs (Feb–Sep 2025 dataset)
https://www.theplakhovgroup.ca/detailed-briefs/trade-war-interactive-visualizations



Your opinions…