
You are currently browsing the tag archive for the ‘Transgender ideology’ tag.
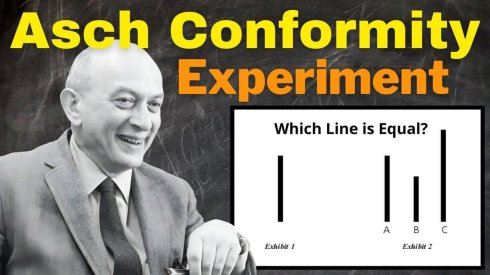
Solomon Asch’s conformity experiments were brutally simple. One person sits with a unanimous group. Two lines of obviously different lengths appear. The group confidently gives the wrong answer. Around 75% of participants conformed at least once. On the critical trials, they went along with the false answer roughly one-third of the time. In the control condition, with no group pressure, errors were almost nonexistent.
That experiment did not stay in the lab.
We now run it as social policy.
A plainly male person enters a female space or female category, and everyone nearby is expected to override what their eyes and judgment are reporting. Not because the evidence is subtle. Because the penalty for stating the obvious has been made artificially high: bigot, transphobe, career risk, social isolation, institutional discipline.
That is the test.
The point is not that everyone believes the lie. The point is that enough people comply in public to make it feel socially mandatory. That is how conformity works: not by proving a falsehood, but by punishing dissent until visible reality becomes something people are afraid to name.
“He knew better. He gave the group answer anyway.”
And the clearer the mismatch, the harsher the demand for submission. Non-passing males are not an embarrassment to this ideology. They are its purest form. They force the conformity trial into the open. The more obvious the contradiction, the more intensely the crowd must insist that you deny it.
Malcolm Gladwell recently handed the game away. Reflecting on his 2022 MIT panel on trans athletes, he admitted he was “ashamed” because he shared Ross Tucker’s position “100%” and was “cowed.” He knew better. He gave the group answer anyway.
That is the real Asch lesson of our time. Social coercion does not need universal belief. It only needs enough fearful public compliance to make reality itself feel socially dangerous.
Call male female, or pay the price.
That is not compassion. It is organized conformity.
Sources:
- Solomon E. Asch, “Opinions and Social Pressure,” Scientific American 193, no. 5 (1955). Classic summary of the line-judgment conformity experiments. Asch reports that in the critical condition, about one-third of judgments shifted toward the erroneous majority, while control-group errors were virtually absent.
- OpenLearn (The Open University), “Starting with psychology: 5.3 Groups and conformity.” Useful summary of Asch’s original findings, including that 75 percent of participants conformed to an obviously wrong answer at least once.
- Encyclopaedia Britannica, “Conformity” and “Normative influence.” Helpful for the distinction your piece relies on: conformity can involve public compliance without private acceptance, which fits your argument that the mechanism is outward submission under pressure rather than sincere belief.
- For the Gladwell reference: The Real Science of Sport podcast follow-up notes confirm that Gladwell apologized for how he handled the 2022 MIT Sloan panel, and contemporaneous reporting quotes him saying he shared Ross Tucker’s position “100%” and was “cowed.”
“Trans kids didn’t exist until we created them” is blunt phrasing, but the mechanism underneath it is real: kids don’t merely reveal identities; they adopt the identity-models a culture supplies and rewards. Adolescence is a meaning-factory. Pain looks for an explanation. Alienation looks for a tribe. If adults and institutions elevate one interpretive story for distress and then attach moral prestige, protection-from-questioning, and instant community to that story we should expect more kids to step into it. Not because every child is “lying,” but because this is how social scripts spread: they simplify suffering, convert it into status, and offer belonging on demand.
Proponents will tell a cleaner story. They claim “trans kids have always existed” and we’re simply seeing higher visibility in a less stigmatizing age. They claim affirmation is harm reduction. They claim the clinical pathway is cautious, selective, and evidence-informed. And they claim the “social contagion” frame is just a pretext to dismiss real dysphoria. That’s the best version of their public narrative: visibility + safety + compassion + careful medicine. The problem is that this narrative asks society to treat disputed assumptions as settled truth and then to treat moral confidence as a substitute for evidence – precisely in the domain where evidence must be strongest: irreversible interventions for minors.
That’s where the ideology runs aground. The evidence base for pediatric medical transition—especially puberty suppression—has repeatedly been assessed as weak and low-certainty. The York-led systematic review published in Archives of Disease in Childhood concluded there is a lack of high-quality research on puberty suppression in adolescents with gender dysphoria/incongruence, and that no firm conclusions can be drawn about impacts on dysphoria or mental/psychosocial outcomes. A 2025 systematic review in the same journal similarly characterized the best available evidence on puberty blockers’ effects as mostly very low certainty. This isn’t a minor academic quibble. It’s the difference between “we have strong reasons to believe this helps, on balance” and “we cannot be confident what this does to developing bodies and minds.” When the confidence level is that low, the ethical default is not acceleration; it’s restraint.
And restraint is exactly what some public health systems have moved toward—because the claims didn’t cash out in robust evidence. In the UK, the NHS stopped routine prescribing of puberty blockers for under-18s and restricted them to research context, and the government moved to make restrictions indefinite after expert advice citing insufficient evidence of safety. NHS England’s Cass implementation materials also frame puberty blockers as part of a research program with long-term follow-up, alongside evaluation of psychosocial interventions. That is not what “settled science” looks like. That is what a field looks like when it is finally admitting—late—that it has been making high-stakes moves on thin ice.
Now zoom out from the clinic to the culture, because this is the part people keep refusing to say out loud: the social environment is not neutral. Once schools, media, and professional bodies moralize one framework (“affirmation is care”) and stigmatize alternatives (“questioning is harm”), you get a one-way ratchet. A child declares an identity; the adults are trained that the declaration must be treated as authoritative; “exploration” becomes suspect if it doesn’t begin with affirmation; and any friction is rebranded as abuse. That moral framing isn’t compassion—it’s epistemic closure. And epistemic closure is exactly how you end up routing heterogeneous adolescent distress into a single explanatory funnel.
Because the presenting population isn’t one thing. It’s a mix: anxiety, depression, trauma, obsessive traits, social contagion dynamics, autism-spectrum features, sexual discomfort, body dysmorphia, internalized homophobia, loneliness, and the general misery of puberty in a screen-soaked status economy. Give that mix one glamorous story with institutional backing, and you will pull more children into it. You will also make it harder for them to exit, because the identity becomes socially defended and medically reinforced. Once irreversible steps begin, doubt becomes expensive. Regret becomes unspeakable. The “care model” becomes self-protecting: the deeper you go, the harder it is to admit the initial certainty was misplaced.
This is why I don’t treat “gender-affirming care” as a neutral phrase. It’s marketing language for a clinical posture that—too often—front-loads conclusion and back-loads caution. Real care for minors under uncertainty looks boring: slow assessment, serious differential diagnosis, treatment of comorbidities, family stability, and time. Real care doesn’t require anyone to be cruel. It requires adults to resist the temptation to turn a child’s distress into an adult moral performance. It requires institutions to stop rewarding certainty and punishing skepticism. It requires the basic humility to say: “We might not know what’s going on yet, and that means we don’t get to make irreversible bets with children.”
If we don’t change course, the end state is predictable. More kids will be swept into an identity pipeline that confers instant meaning but demands escalating commitment. More parents will be coerced by policy and stigma rather than persuaded by evidence. More clinicians will practice defensively in a moralized climate. And the backlash won’t stay polite or surgical; it will arrive as a blunt instrument, because careful critics were dismissed as hateful for too long. That’s the social damage: not merely the trend itself, but the institutional refusal to admit uncertainty until the human costs become impossible to ignore.
![]()
At the core of much of the tension surrounding transgender issues lies a profound and inescapable cognitive dissonance.
P
Biological reality is clear and immutable.
P
Human sex is binary—male or female—and determined at conception. No medical intervention, no amount of social affirmation, and no subjective feeling can change this fundamental fact. You will always and forever remain the sex you were born.
P
Transgender ideology asserts the opposite. It claims that whatever sex you feel you are, you become in reality. Your internal sense of self overrides chromosomes, reproductive anatomy, and every observable marker of biological sex. This ideology is inherently anti-reality.
P
Those who fully internalize it place themselves in a state of permanent conflict—not just with their own bodies, but with the entire external world. Reality itself becomes the enemy, repeatedly negating their subjective self-perception.
P
Queer Theory provides the escape hatch. Rather than confronting the mismatch between feelings and facts, adherents are guided to externalize the source of their distress. Through an oppressor/oppressed lens, the cause of their pain is never their own faulty perception of self—absolutely not. Instead, it is “normative” society that is actively oppressing them, enforcing rigid gender norms and inflicting all their suffering. This framework transforms personal dissonance into righteous grievance. The distress is no longer internal; it is the fault of everyone else.
P
Medical interventions amplify the problem. So-called “gender-affirming care”—puberty blockers followed by cross-sex hormones—adds fuel to the fire. These treatments carry serious, well-documented deleterious effects on both mental and physical health. Far from resolving underlying issues, they often deepen psychological instability while creating permanent physical changes.
P
The result is a perfect storm: individuals who were already vulnerable, now further destabilized, carrying a massive chip on their shoulders. They view the rest of society—the “normative” majority—as the active source of their pain. To defend their constructed identity and quiet the cognitive dissonance, they feel compelled to strike back against this perceived evil force: you and me.In this worldview, disagreement equals enmity.
P
If you refuse to affirm their ideology, you are not offering a different opinion—you are the oppressor who must be confronted, silenced, or defeated.
P
Dissent is violence.
P
Reality itself is violence.
P
This dynamic helps explain patterns of hostility, aggression, and, in extreme cases, violence that emerge from certain segments of transgender activism. It does not stem primarily from societal rejection, but from a foundational rejection of biological reality and the refusal to address internal distress with honesty.
True compassion does not mean enabling delusion.
P
It means grounding support in reality—the only place where genuine mental health and social peace can be found.
The rapid proliferation of gender ideology over the past decade—especially the surge of adolescent-onset gender dysphoria—stands as one of the clearest examples of social contagion in modern Western societies. A clinical framework once reserved for a very small number of adults with persistent, childhood-onset dysphoria was transformed into a cultural mandate through the convergence of three forces: institutional capture, algorithm-driven identity formation, and activist-driven medical practice.
Between 2015 and the early 2020s, referrals for gender services exploded—driven overwhelmingly by teenage girls with no prior history of dysphoria. Peer-group clustering, sudden identity shifts following intense online exposure, and the complete inversion of historic sex ratios all point to a socially transmitted phenomenon rather than a newly discovered biological one. Yet under the “affirmation” model, minors were placed on puberty blockers, cross-sex hormones, and permanent surgeries despite limited evidence, poorly understood risks, and a professional culture that increasingly discouraged clinical skepticism.
The hardest obstacle to unwind, however, will not be the institutions that enabled this shift. Policies can change, clinics can be restructured, and professional bodies can revise guidelines—as they already have across parts of Europe. The most immovable barrier will be parents. Many acted from compassion, social pressure, or a sincere desire to be “supportive,” but they now face an excruciating truth: they approved irreversible medical interventions on psychologically vulnerable teenagers during a developmental window historically marked by transient distress, identity confusion, and social sensitivity.
Double mastectomies on minors, lifetime fertility loss, and surgeries with complication rates exceeding anything considered acceptable elsewhere in medicine are not abstract debates. They are lived consequences. For parents, acknowledging error would require confronting a moral reality few can bear: that they were active participants in harming their own child. The human mind is built to avoid that revelation at all costs.
As a result, the detransition wave—real, growing, and increasingly documented—will face its fiercest resistance not from clinics or activists, but from within families. Parents will cling to the “lifesaving care” narrative long after the institutions that encouraged it have quietly retreated. They will reinterpret events to preserve psychic stability, even if doing so deepens the suffering of the child who must now live with the consequences.
Reversing the damage will require more than policy reform or legal accountability. It will require a public reckoning with the psychological mechanisms of self-deception, moral injury, and sunk-cost loyalty that allowed an entire society to medicate and operate on distressed adolescents in the name of affirmation. That reckoning—private, painful, and unavoidable—is the hardest part still to come.

References
-
The Cass Review – Independent Review of Gender Identity Services for Children and Young People (Interim Report) — NHS-commissioned review (Feb 2022) by Dr. Hilary Cass. Sex Matters
-
The Cass Review: Final Report (April 2024) — Hilary Cass’s full independent review. BASW+1
-
NHS England: Public Consultation Analysis & Summary – Interim Clinical Policy on Puberty-Suppressing Hormones (Jan 2024) — analysis of feedback on proposed policy changes. NHS England
-
Commission on Human Medicines (UK) Report – Proposed Restriction on GnRH Agonists for Under-18s — recommendation to restrict puberty blockers. GOV.UK
-
Equality & Health Inequalities Impact Assessment (EHIA), NHS England — assessment of health-inequality risks from the policy change on puberty blockers. GOV.UK+1
-
Karolinska Institutet Systematic Review on Hormonal Treatment in Youths (<18) — finds that GnRHa treatment should be considered experimental due to lack of long-term data. Karolinska Institutet News
-
Karolinska Hospital Policy Statement (April 2021) — stops prescribing puberty blockers and cross-sex hormones to minors under 16 except in research settings. Feminist Legal Clinic
People should be consistent about their beliefs. Let’s put a bodily autonomy situation to the test.
-
Major Premise: Any moral principle protecting a woman’s bodily autonomy and safety must be applied consistently to all areas where her biological sex is directly relevant.
-
Minor Premise 1: Abortion rights protect a woman’s bodily autonomy.
-
Minor Premise 2: Female-only spaces protect a woman’s safety and dignity, which are inseparable from her biological sex.
-
Conclusion: Therefore, just as abortion is morally protected for bodily autonomy, the right of women to control access to female-only spaces must also be morally protected
Let’s consider a possible counter –
-
Trans inclusion claim: Some argue trans women should access female spaces.
-
Counterpoint: Biological sex, not gender identity, determines risk factors (e.g., privacy violations, physical safety concerns), which are the basis for female-only spaces. Moral protection of women’s autonomy and safety therefore cannot be overridden by gender identity claims.
This (and logic generally) only works if you belief in objective truth and a shared common reality. Social constructivists are bound by neither, so this argument probably wouldn’t work well with them.


The notion of LGB/TQ+ ‘community’ is in itself a synthetic proposition. How do people who share mutually exclusive goals reasonably be part of the same “community”? LGB are about acceptance into society based on sexual attraction preferences – that is if you happen to like the same sex you should be able to pursue your life without facing discrimination for doing so. The TQ+ doesn’t believe in sex at at all, and are not about fitting into society – they are there to burn down the old society and reformat society’s rules and norms according to their ideology – aka – the entire transgender campaign that denies the reality of sex in humans and reifies the notion of mystical gender identity. The fetish driven men in dresses need to justify their paraphilia and thus children must also be transed and mutilated/sterilized in the name of gender ideology.
We must keep in mind that “queer” isn’t a identity you are. You can act queer and do queer things but queer is an identity without an essence – queer exists only in opposition to the norm and by definition is a political identity(one that seeks to destroy the current society).
Anyhow, here in the West the scales have been tipped far to long in the queer activists’s favour. People in the US (and hopefully soon in Canada) have rejected the activism and are now rolling back the damage done to society by self righteous activists who have been happily corroding society for years. The pendulum swinging back is causing some consternation in the LGB/TQ+ community.
Here is a notable ‘activist’ now blaming the human shields she used to advance her activism for the backlash she is responsible for.

This is a masterclass level response:

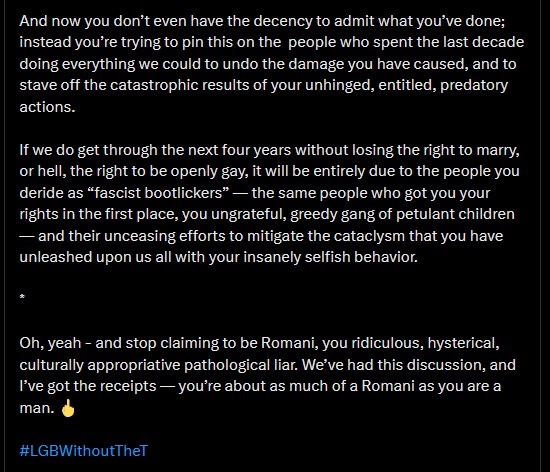
Hard to disagree with any of the points made. We should all be taking notes on how this happened as this is how activists work in the West – they get on the inside and corrupt institutions with their bullshit and then ruin the party for everyone involved.



Your opinions…