If you would like to learn more about Therapy First, to support our work, or to find a therapist for you or your child, please reach out: www.therapyfirst.org. Go to their website and check them out – they are mental health resource that puts therapy instead of the farce that is gender affirming care in the spotlight.
I have been a practicing psychologist for over two decades and this is, by far, the most difficult work I have ever engaged in. I can understand why many therapists do not feel equipped to work with young people who are convinced that the only way for them to live in their bodies is to transition socially and medically.
It is challenging to sustain a meaningful connection with someone who is stuck in a black/white mindset and who is exquisitely attuned to whether you participate in the culture and language of social justice and gender affirmation.
Depending on how committed an individual is to a transgender identity, he or she may not tolerate the slightest indication that the therapist questions or is agnostic with regard to the existence of “true trans”. They may see you as a good, kind, caring person for months and then, if in a moment of crisis, they don’t perceive you to be fully aligned with their belief system, they will reject you without hesitation.
At the same time, frightened and exhausted parents are putting their faith in you to loosen the vice-like grip that trans identification has on their child and, by extension, on every member of the family. Having been such a parent myself I feel enormous empathy.
I also know that most of the work has to happen at home, in the family. I am more than willing to offer guidance and support, and even clear instructions in real time on what to do and say when escalations happen.
When things go wrong, what rage parents and children cannot safely direct at each other will get directed at me. As a process-oriented clinician that’s what I sign up for.
In truth, I don’t possess skills or knowledge that any well-trained and experienced mental health practitioner doesn’t have or isn’t capable of acquiring. Therapy is still just therapy.
What’s different is the real damage that medicalized transition can do to young people who are in emotional pain and in need of thoughtful care and attention. What’s also different is the urgency with which families approach us hoping we might hold the key to pulling their children out of harm’s way. There’s so much on the line.
Clinicians who work with trans-identifying teens and young adults feel a pressure that we do not experience when faced with other issues that are no less serious than gender dysphoria. Moreover, we are doing this work in a professional and political climate that is hostile to the very ethical principle that we vow to live and work by, to first and foremost do no harm.
The good news is that since its establishment three years ago Therapy First (formerly GETA) has grown from a small handful of clinicians to now almost 400 strong. We are here for each other so that we can be there for you and your family. While the treatment of gender dysphoria has become weaponized, our aim is to move the focus away from the political and back to the clinic, back to the work we are confident and passionate about.
If you would like to learn more about Therapy First, to support our work, or to find a therapist for you or your child, please reach out: www.therapyfirst.org.
I was a strong proponent of the Harm Reduction strategy until more data has come out about its effectiveness and benefits for society versus other methods. There might be a case for Harm Reduction, but as currently implemented in BC it is a like a 4 legged stool that is missing three legs -harm reduction, law enforcement, prevention and treatment – just focusing on harm reduction and not the other areas is a recipe for social disaster.
The Alberta rehabilitation model has been modestly more successful in dealing with the problems of addictions. Both systems require overlapping programs working together to get people out of the drug abuse loop – whether Alberta has been more successful in coordinating the synergy of anti-addiction programs or that rehabilitation programs are just more effective remains to be seen. Initial data points to the Alberta method being more successful.
The divergent policies and politics of B.C. and Alberta have played a major role in determining the public perception of Canada’s opioid crisis. Left-leaning media outlets have tended to laud B.C.’s harm reduction as being more compassionate, while conservative voices point to Alberta’s focus on treatment as more practical and realistic. What Canada had lacked until recently was an impartial, data-driven assessment of the two competing systems.
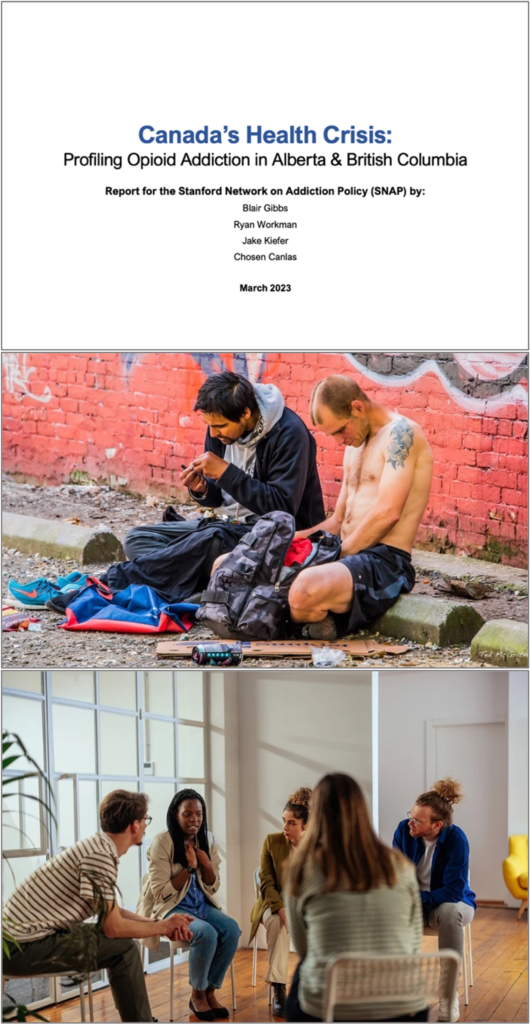
Advantage Alberta: The Stanford Network on Addiction Policy’s 2023 report (depicted above) observes that, “Alberta is currently experiencing a reduction in key addiction-related harms,” while “Canada overall, and BC in particular, is not yet showing the progress that the public and those impacted by drug addiction deserve.” At middle, a typical street scene in Vancouver’s Downtown Eastside; at bottom, a therapy session at Alberta’s new Red Deer Recovery Community. (Sources of photos: (middle) Ted McGrath, licensed under CC BY-NC-SA 2.0 DEED; (bottom) EHN Canada)
That problem was partially solved last year with the release of a report from the U.S.-based Stanford Network on Addiction Policy. Entitled Canada’s Health Crisis: Profiling Opioid Addiction in Alberta & British Columbia, the document offers an even-handed review of the differing policies of the two provinces, summarizes the latest available data (which it criticizes as inadequate) and cautiously evaluates the results. B.C., the report notes, emphasizes harm reduction, “safe supply” of illicit drugs, decriminalization of possession and reduction of addiction stigma. Alberta, by contrast, is focusing on “investment in rehabilitation beds and spaces, such as therapeutic communities,” while moving away from “safe supply” of opioids and instead providing addicts with medications.
Using these differences as a natural experiment, the Stanford report comes to a few key conclusions. First, it observes “a lack of policy innovation in BC on the issue of drug addiction.” Obsessive attention to harm reduction appears to have blinded politicians and public health officials to the longer-term consequences of their favoured policy. “Enforcement against drug crime has [been] reduced in recent years,” the report notes, “indicating a general lessening of criminal justice enforcement against drug offences in Canada during the escalating health crisis of opioid addiction.”
Second, “Of the two provinces studied for this report, Alberta is currently experiencing a reduction in key addiction-related harms.” The province’s rate of overdose deaths declined by 17 percent from 2021 to 2022 (B.C.’s remained almost unchanged), although it was still Alberta’s second-worst year on record. Using the most recent data available, the Stanford researchers point to B.C.’s higher death rate as suggestive of the two approaches’ relative effectiveness: “Our research indicates that Canada overall, and BC in particular, is not yet showing the progress that the public and those impacted by drug addiction deserve.”
The very real threat of nuclear war hasn’t been on the radar since the fall of the Berlin Wall in 1989. Yet the capacity for self-annihilation remains. Consider the question raised by Daniel Ellsberg:
“When I say that there is a step that could reduce the risk of nuclear war significantly that has not been taken but could easily be taken, and that that is the elimination of American ICBMs, I’m referring to the fact that there is only one weapon in our arsenal that confronts a president with the urgent decision of whether to launch nuclear war and that is the decision to launch our ICBMs.”
He went on to stress that ICBMs are uniquely dangerous because they’re vulnerable to being destroyed in an attack (“use them or lose them”). In contrast, nuclear weapons on submarines and planes are not vulnerable and
“can be called back — in fact they don’t even have to be called back, they can… circle until they get a positive order to go ahead… That’s not true for ICBMs. They are fixed location, known to the Russians… Should we have mutual elimination of ICBMs? Of course. But we don’t need to wait for Russia to wake up to this reasoning… to do what we can to reduce the risk of nuclear war.”
And he concluded: “To remove ours is to eliminate not only the chance that we will use our ICBMs wrongly, but it also deprives the Russians of the fear that our ICBMs are on the way toward them.”
It would be a great step toward securing the world from a nuclear extinction level event, but the geopolitics of the situation make the move a contested one at best.
If the death of everyone can still be maintained with bombers and submarines do we really need the extra death (and extra threat) of ICBM’s? Is it even rational to consider the move as it might embolden the Russians and Chinese with even the perceived move away from MAD?
It is a calculus that makes sense in terms of lowering the threat to the entire world, but are the corresponding consequences (real or perceived) worth the risk, as it would have to be the US that would stand down first.
“Ramer asked Turban to explain the GRADE method (Grading of Recommendations Assessment, Development and Evaluations), a standardized EBM framework for evaluating quality. “GRADE generally involves looking at the research literature,” Turban explained. “And then there’s some subjectivity to it, but they provide you with general guidelines about how you would—like, great level of confidence in the research itself. Then there’s a—and then each of those get GRADE scores. I think it’s something like low, very low, high, very high. I could be wrong about the exact names of the categories.” Turban is indeed wrong: the categories are high, moderate, low, and very low. It’s surprising that someone involved in the debate over gender-medicine research for several years, and who understands that questions of GRADE and of quality are central, doesn’t know this by heart.
Ramer asked Turban what method, if any, he uses to assess quality in gender-medicine research. Turban explained that he reads the studies individually and does his own assessment of bias. GRADE is “subjective,” and this subjectivity, Turban said, is one reason that the U.K. systematic reviews rated studies that he commonly cites as “very low” quality. Turban’s thinking seems to be that, because GRADE is “subjective,” it is no better than a gender clinician sitting down with individual studies and deciding whether they are reliable.
I asked Guyatt to comment on Turban’s understanding of systematic reviews and GRADE. “Assessment of quality of evidence,” he told me, “is fundamental to a systematic review. In fact, we have more than once published that it is fundamental to EBM, and is clearly crucial to deciding the treatment recommendation, which is going to differ based on quality of evidence.” Guyatt said that “GRADE’s assessment of quality of the evidence is crucial to anybody’s assessment of quality of evidence. It provides a structured framework. To say that the subjective assessment of a clinician using no formal system is equivalent to the assessment of an expert clinical epidemiologist using a standardized system endorsed by over 110 organizations worldwide shows no respect for, or understanding of, science.”
At one point, Ramer pressed Turban to explain his views on psychotherapy as an alternative to drugs and surgeries. Systematic reviews have rated the studies Turban relies on for his support of puberty blockers and cross-sex hormones “very low” quality in part because these studies are confounded by psychotherapy. Because the kids who were given drugs and improved were also given psychotherapy and the studies lack a proper control group, it is not possible to know which of these interventions caused the improvement.
Turban seemed not to grasp the significance of this fact. If hormonal treatments can be said to cause improvement despite confounding psychotherapy, why can’t psychotherapy be said to cause improvement despite confounding drugs?
The exchange about confounding factors came up in the context of Ramer asking Turban about an article he wrote for Psychology Today. The article, aimed at a popular audience, purports to give an overview of the research that confirms the necessity of “gender-affirming care.” Last year, I published a detailed fact-check of the article, showing how Turban ignores confounding factors, among other problems. Four days later, Psychology Today made a series of corrections to Turban’s article. Some of these corrections were acknowledged in a note; others were done without any acknowledgement. In the deposition, Ramer asked Turban about my critique, to which Turban replied that he “left Psychology Today to do whatever edits they needed to do,” and that, when he later read the edits, he found them “generally reasonable.”
In sum, though Turban says that “there are no evidence-based psychotherapy protocols that effectively treat gender dysphoria itself,” the same studies he cites furnish just as much evidence for psychotherapy as they do for puberty blockers or cross-sex hormones—which is to say “very low” quality evidence.”
The quality of evidence that Gender Affirming Care works is “Very Low”. In other words those who argue for Gender Affirming Care are arguing from a base of low quality, probably confounded evidence that doesn’t say what they think it says. It just another example of how the pseudo-science of gender identity is propagated by believers – even medical doctors – over the principles of evidence based medicine. Make sure you go and read the full article, it is a wild ride.
The gender cult and associated gender religious members are pushing bullshit and now, finally, the stink is starting to seep out.
The truth about transgender ideology as always been there, it has just been that people have been too afraid to speak out against it. The tide is turning.
On Feb 21, 2023 the Florida House Health & Human Services Committee heard testimony from licensed psychiatrist Stephen Levine MD. He outlined 13 scientifically false assumptions which serve as the foundation of affirmation-only therapy for gender dysphoria in kids.
00:00 Stephen Levine Presentation
00:08 The 13 Untruths of Gender Ideology
01:10 Medical Misadventures
02:04 1 – A Trans Identity is immutable and unchanging
02:14 2 – A Trans Identity is rooted in biology
02:28 3- Gender Identity has no connection to sexual orientation
03:18 4 – No form of Gender Identity is a symptom of something else
03:38 5 – Gender dysphoria is a serious medical condition requiring intervention or not
04:01 6 – Associated emotional problems are due to discrimination
04:17 7 – There are no effective alternatives to affirmative care
04:40 8 – Exploratory psychotherapy is conversion therapy
04:59 9 – Affirmative Care improves mental health and social function in the long term
05:30 10 – Affirmative Care prevents suicide
06:24 11 – Teens know whats best for themselves
06:39 12 – Meeting diagnostic criteria for gender dysphoria predicts good outcome
06:51 13 – Regret and detransition are rare
07:27 Conclusion
What is ad block? It is an application that, at your discretion blocks out advertising so you can browse the internet for content as opposed to ads. If you do not have it, get it here so you can enjoy my blog without the insidious advertising.





Your opinions…