
You are currently browsing the tag archive for the ‘Gender Ideology’ tag.
The recent ruling against Amy Hamm by the British Columbia College of Nurses and Midwives (BCCNM) is nothing short of a travesty, a glaring assault on free speech and common sense that should leave any reasonable person fuming. Hamm, a nurse and vocal advocate for women’s sex-based rights, was found guilty of “professional misconduct” in March 2025 for stating biological facts and expressing opinions critical of gender identity ideology. Specifically, the disciplinary panel zeroed in on a handful of her online statements—made while identifying as a nurse—deeming them “discriminatory and derogatory” toward transgender individuals. This isn’t just a punishment for Hamm; it’s a warning shot to every professional in Canada: step out of line with the prevailing ideology, and your career could be next. How dare a regulatory body, meant to ensure competence in healthcare, stretch its tentacles into policing personal beliefs expressed off-duty?
What’s particularly infuriating is the absurdity of the tribunal’s reasoning—or lack thereof. One so-called expert reportedly argued that being a woman is a “social identity category rather than a biological reality,” a statement so detached from science it’s laughable if it weren’t so dangerous. Hamm’s crime? Asserting that biological sex is real and matters, especially when it comes to women’s spaces and rights—a position grounded in observable fact, not hate. Yet, the panel chose to side with ideological fantasy over evidence, slapping Hamm with a guilty verdict for daring to speak her mind. This isn’t about protecting anyone; it’s about control, about silencing dissent under the guise of professionalism. The fact that her extensive Twitter posts, where she didn’t explicitly tie her nurse status, were spared only highlights the flimsy, cherry-picked nature of this witch hunt.
The implications of this ruling are chilling, and that’s putting it mildly. If a nurse can be professionally crucified for advocating for women’s rights and biological truth, what hope is there for free discourse in Canada? The BCCNM’s decision doesn’t just harm Hamm—it erodes the freedom of every regulated professional, from doctors to teachers, who now must tiptoe around controversial issues or risk their livelihoods. This is the kind of dystopian overreach that should spark outrage, not apathy. Hamm’s fight isn’t over—she’s hinted at appeals, potentially up to the Supreme Court—and thank goodness, because someone needs to stand up to this madness. We should all be rooting for her, not because we agree with every word she says, but because the principle at stake is too precious to let slip away without a fight.

Hegel’s assertion in modern times:
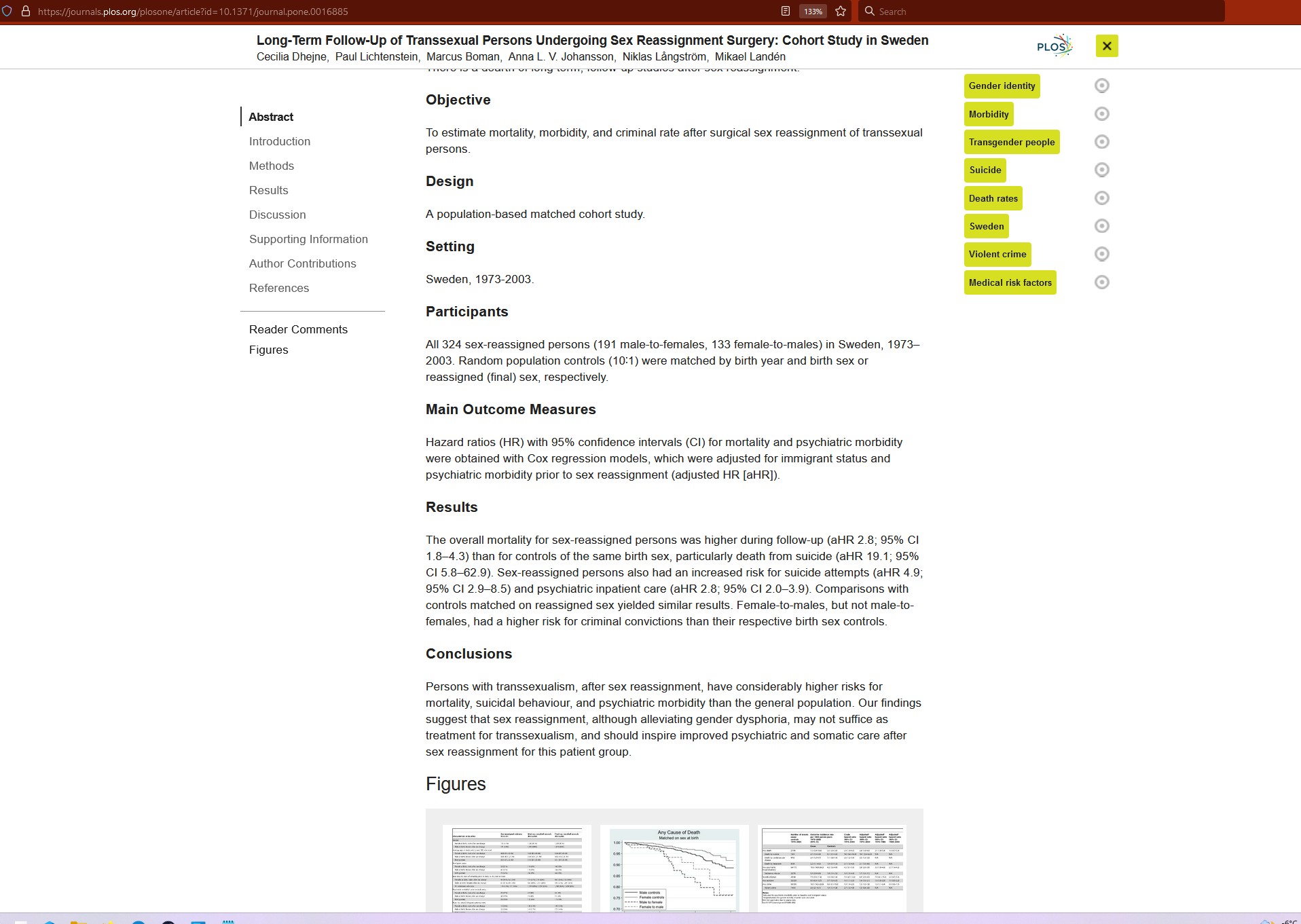
If there was such a thing as a “female brain trapped in a male body” that demographic group would exhibit a criminal offending pattern consistent with that of women rather than men.
We’ve had data since 2011 showing that men who have their genitals surgically removed and take cross-sex hormones continue to exhibit the same criminal offending pattern as all other men.
Humans cannot change sex and no human was ever born “trapped in the wrong body.”
Assuming we don’t have empathy for them is decidedly uncharitable.
Where is that young woman’s empathy for women and little girls who don’t deserve to be subject to sex crimes in female spaces?
Voyeurism is illegal for good reason and nobody can legalize it or make sexual consent decisions on anybody else’s behalf about who is allowed to see us naked.
Summary
This editorial describes the Cass Review findings and the extraordinary challenge we all face in managing uncertainty amid a toxic and highly polarised debate. Children and young people will only get the best care if patients and professionals join forces to seek answers collaboratively and respectfully.
‘Medicine’s ground state is uncertainty. And wisdom – for both the patients and doctors – is defined by how one copes with it.’ Reference Gawande1
In April 2024 I published the final report of my 4-year independent review (Review) of gender identity services for children and young people.Reference Cass2 It is a report about uncertainty, complexity and the need to listen, to learn and above all to discuss and collaborate.
Multiple different truths exist within this space, and views are often more aggressively voiced than in any other area of clinical care, such that many people are afraid to express an opinion; this is a dangerous situation for both doctors and patients. Indeed, in my 40 years of medical practice it proved to be the first time that it was not even possible to get individuals with the most polarised views into a room together.
In this editorial I discuss some of the most difficult dilemmas I encountered, which underpin the profound disagreements and emotional responses to this topic. However, as stated in the final report, while open and constructive debate is needed about the findings of the Review and its recommendations, everybody should remember the children and young people trying to live their lives and the families/carers and clinicians doing their best to support them. All should be treated with compassion and respect.
The review’s approach
The bedrock of the Review was a series of seven systematic reviews commissioned from the University of York, as well as a survey of international practice and a qualitative study examining the range of experiences and outcomes of patients, and the perspectives of parents/carers and clinicians.
The systematic reviews are the largest and most comprehensive to date. The use of a single search strategy across all the reviews was more inclusive than any previous systematic reviews, capturing 237 papers from 18 countries, and providing information on a total of 113 269 children and adolescents.
In this area where views are polarised and uncertainty abounds, it was crucial that there was access to expert experience and opinion to contextualise the emerging evidence. Therefore, in addition to the commissioned work from the University of York, a mixed-methods engagement approach was taken that prioritised two categories of stakeholders: first, people with relevant lived experience (direct or as a parent/carer) and organisations working with LGBTQ+ children and young people generally. Second, clinicians and other relevant professionals with responsibility for providing care and support to children and young people.
Overall, those conducting the Review met with over 1000 individuals, some in one-to-one meetings, some in bespoke meetings on a particular topic and others in meetings focused on building awareness and improving understanding of the issues among interested parties and organisations.
Dilemma 1: understanding the population
The population of young people presenting to gender services in recent years is markedly different from those who presented 10–15 years ago. At that time, the service offered a therapeutic model of care, and most patients were pre-pubertal birth-registered males presenting with gender incongruence from early childhood. A minority had persisting gender incongruence and were offered masculinising or feminising hormones from age 16, while the majority grew up to be same-sex attracted cis adults.
From about 10 years ago, there was a dramatic rise in the numbers presenting to the Gender Identity Development Service (GIDS) at Tavistock & Portman National Health Service (NHS) Trust, which was the only specialist service for patients in England, Wales and Northern Ireland. Referrals increased from less than 50 per annum before 2009 to around 2500 by 2019. The case mix also changed to largely birth-registered females presenting in early teenage years, with additional complex problems including a history of trauma or adverse childhood experiences, depression, anxiety, neurodiversity and a range of psychosocial issues.
Based on the evidence and on discussion with clinicians and academics, the Review took the view that this is a heterogeneous population of young people, and that a complex mix of biopsychosocial factors, unique to each individual, was responsible for their gender incongruence or distress. Some would continue to have a stable trans identity into adulthood and would benefit from medical transition. For others, the gender-related distress might be a transient phenomenon during a dynamic period of personal and psychosexual development and might resolve in late teens or young adulthood. The conclusion of this analysis was that there could not be a ‘one size fits all’ approach, and that each individual would need a holistic assessment and a personalised care plan.
This conceptualisation of the population is one of the first areas of disagreement from which much of the polarisation arises. A 2015 studyReference Vrouenraets, Fredriks, Hannema, Cohen-Kettenis and de Vries3 approached 17 multi-professional treatment teams worldwide to determine their views on the use of early intervention with puberty blockers. They identified seven themes on which there were widely disparate views, with two being fundamental to attitudes to treatment: ‘the (non-) availability of an explanatory model for gender dysphoria’ and ‘the nature of gender dysphoria (normal variation, social construct or [mental] illness)’.
During the course of the Review, we observed a change in attitudes, from an initial narrative among many trans advocates that only a minority of the young people presenting would have a longstanding trans identity and would benefit from a medical pathway to a belief in some quarters that all the young people on the waiting list for services were ‘trans kids’.
The Review spoke to young people and adults who had longstanding gender incongruence and had gone through a successful medical transition, with positive experiences of the treatment pathway. The team also spoke to individuals who had gone through a period of trans identification that had completely resolved in late teens and/or early adulthood. Neither of these experiences should invalidate the other.
The challenge lies in the lack of a reliable way of predicting the trajectory of any one individual and hence the right approach to treatment.
Dilemma 2: role of puberty in psychosexual and identity development
That puberty and adolescence are times of rapid change, development and emotional challenge is beyond dispute. During this period body image becomes a major preoccupation and can have either positive or negative impacts on mental health. Young people start to explore their sexuality and to understand their sexual orientation. Peers have an increasing influence and parents a lessening influence.
The practice of pausing puberty at Tanner stage 2 was initiated in the Netherlands, and subsequently adopted in the UK and internationally. The idea was based on a theory from Dr Peggy Cohen-Kettenis, whose initial clinical experience was in adult care. Her rationale was that pausing puberty early would help young people to ‘pass’ better in adulthood and ‘extend the diagnostic period’ by buying time to think. The use of puberty blockers for this purpose was initially reported in a single case study and then in the original Dutch cohort,Reference de Vries, Steensma, Doreleijers and Cohen-Kettenis4 which had tightly defined inclusion criteria: patients had to be a minimum age of 12, have gender dysphoria from childhood, increasing around puberty, be psychologically stable without serious comorbid psychiatric disorders that might interfere with the diagnostic process and have family support. The Dutch group found some modest improvements in mental health in a pre–post study without a comparison group, but no impact on gender dysphoria or body satisfaction.
In 2011, the GIDS early intervention study was launched in the UK in an attempt to replicate the findings of the Dutch team. This was an uncontrolled prospective observational study of the use of puberty blockers. Preliminary results from the early intervention study in 2015–2016 did not demonstrate benefit. Some 98% of the cohort went on to masculinising or feminising hormones. The results of the study showed a lack of any positive measurable outcomes but were not released until the day after the Bell versus Tavistock judgment in December 2020, and were eventually published in 2021.Reference Carmichael, Butler, Masic, Cole, de Stavola and Davidson5
Despite this, from 2014, puberty blockers moved from a research-only protocol to being available in routine clinical practice and were given to a broader group of patients with later onset of gender-related distress who would not have met the inclusion criteria of the original protocol. An audit carried out for the Review looked at records of patients who had been discharged from GIDS between 1 April 2018 and 31 December 2022 and found that over half of the young people prescribed puberty blockers started this medication between 15 and 16 years old, raising questions about the treatment goals at this late stage of puberty.Reference Cass2
The University of York systematic reviewReference Taylor, Mitchell and Hall6 found no evidence that puberty blockers improve body image or dysphoria, and very limited evidence for positive mental health outcomes, which without a control group could be caused by the placebo effect or concomitant psychological support. Indeed, given that hormonal surges are a normal part of puberty and are known to lead to mood fluctuations and depression, it is not unexpected that blocking these surges may dampen distress and improve psychological functioning in the short term for some young people.
The adoption of a treatment with uncertain benefits without further scrutiny is a significant departure from established practice. This, in combination with the long delay in publication of the results of the early intervention study, has had significant consequences in terms of patient expectations of intended benefits and demand for treatment.
This leaves many unanswered questions, including whether puberty blockers may be beneficial for a subgroup of young people, and if so which ones, as well as whether there might be negative outcomes for other young people.
A recent study found that gender non-contentedness (i.e. unhappiness with being the gender aligned with one’s sex) was highest in early adolescence and continued to drop into the mid-20s.Reference Rawee, Rosmalen, Kalverdijk and Burke7 This is consistent with accounts shared with the Review by people with lived experience whose gender-related distress resolved in late teens or early adulthood. If pubertal changes are essential to both psychosexual development and resolution of gender-related distress in some individuals, does treatment with puberty blockers change the trajectory for that group? Unfortunately, because we have intervened with the later-presenting group by using a treatment that was intended for those presenting in early childhood, and in the absence of an evidence base, we do not know what their natural history would be, nor the appropriate treatment response.
In light of all these uncertainties, the Review recommended that a puberty blocker trial should be established as part of a wider programme of research, and NHS England and the National Institute for Health and Care Research (NIHR) have already initiated this process.
Dilemma 3: weakness of the evidence base informing treatment decisions
The weakness of the evidence base was not limited to treatment with puberty blockers. Across the suite of systematic reviews, the evidence base underpinning both medical and non-medical interventions was remarkably weak compared to other areas of paediatric practice. This was particularly striking in the context of prescription of life-changing medications. The majority of studies had problems such as inadequate follow-up periods, high attrition rates, inappropriate or unclear comparison groups and confounding interventions, limiting the conclusions that could be drawn. The full systematic review series is available here: https://adc.bmj.com/pages/gender-identity-service-series.
The Review discussed the high-profile legal cases that have considered the question of whether young people have the capacity or competence to consent to medical treatment for gender dysphoria. However, capacity or competence is only one part of the process underpinning informed consent. Clinicians are responsible for the prescriptions they sign, so before offering a treatment they must make an adequate assessment to determine whether the drug serves the patient’s needs; this is made more difficult in this area because we do not have good predictive tools to determine which young people will benefit from medical intervention, and which might not. The clinician should also ensure that the patient is fully informed about the risks and benefits of the intervention and, again, the weak evidence base makes it difficult to provide the patient with reliable information.
One of the most challenging difficulties in discussing options with young people is the lack of information about the longer-term outcomes of different treatments. Because this information is not available for interventions in this group of children and young people, a strand of research commissioned by the Review was a data linkage study. The aim of this study was to fill some of the gaps in follow-up data for the approximately 9000 young people who have been through GIDS. The study received full ethical approval, as well as patient and public involvement support, but unfortunately the refusal of the adult gender services to cooperate meant that the research was not possible.
Moving forward in the face of uncertainty
The Review made 32 recommendations about how best to provide services for this group of children and young people. Most of the recommendations were focused on bringing care back in line with the usual standards and processes that are fundamental to good clinical practice.
Core to the recommended approach is the development of a networked group of regional hubs in tertiary paediatric centres, working in close collaboration with local mental health and paediatric teams. By working in a partnership model with a strong focus on education, clinical improvement and research, the goal will be to provide a holistic model of care as close to home as possible, while upskilling the workforce and addressing some of the unresolved research questions set out above.
The healthcare system inadvertently exceptionalised this group of children and young people, placing them on a waiting list for a single specialist service that was not equipped to deal with the full range of their difficulties. This has come about in no small part because clinicians have been disempowered. Many are afraid to conduct the assessments that they would undertake for any other young person, to diagnose other relevant conditions such as neurodiversity and to offer the evidence-based treatments that could help them with their anxiety, depression, trauma or other psychosocial stressors.
If we are to do better for children and young people with gender-related distress, there must be an end to hostile and aggressive discourse, a coming together of professional organisations and the humility to acknowledge the limits of the science and that no one has all the answers. We must also recognise that this is a group of young people who share all the same aspirations, joys, emotional growing pains, triumphs and traumas as every other adolescent, and respond accordingly.
Declaration of interest
H.C. is chair and author of the Independent Review of Gender Identity Services for Children and Young People: Final Report.Reference Cass2
I cannot vote for a party that is favour of undermining parents’ relationship with their children, and a party that is favour of putting children on medical pathways that lead to sterilization and life long medicalization.

Then the Leader of the NDP decides to hide replies like this:
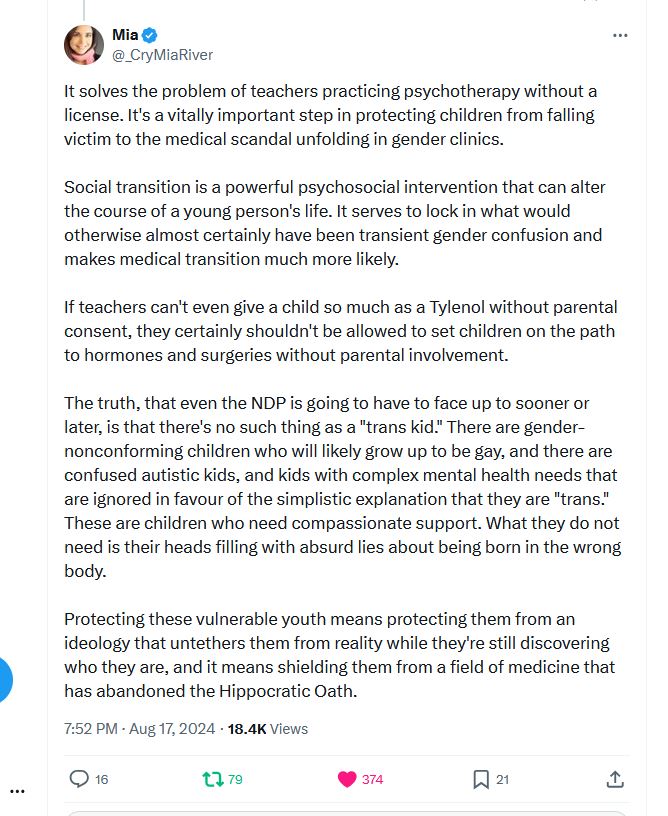
Nope, nope, nope. We can’t have people who major in medical science denial anywhere near the levers of power.
Nothing gets the juices flowing more than a little woke hypocrisy in the afternoon. Scrolling through facebook I saw a post for a choral get together with the goal of showing “the transphobes” how wrong they are.
My first reaction was one of exasperation because the individual who uttered it is currently kicking up a huge fuss in the choral community. The reason? She got in a disagreement with the conductor about whether wearing a “they/them” pronoun pin on stage was acceptable part of the dress code for a professional choir.
Pro-tip: It’s not. And she wouldn’t let it go – so Fing around and finding out involved not having her contract renewed with said professional choir. Play stupid games and win stupid prizes. Unfortunately, as it is with so many of the Woke zealots, she has an activist bent and has been wailing about how oppressive the decision was and how the ‘ENTIRE ORGANIZATION’ is transphobic. This is the standard tactic for the woke activist – you call something/someone transphobic until they relent to your demands or the organization crumbles. It’s bullshit and I hope the professional choir as the fortitude to withstand the struggle session it is being put through.
“They/them” othered their ideological opponents in a public comment and I found that to be infuriating because there is no sense of fairness in the statement. “Othering” is a one way problem.
People that meltdown when people are “othered” shouldn’t participate in the othering of their ideological opponents. Calling people you disagree with “transphobes” illustrates the strong lack of an ethical system behind followers of gender ideology.
So many people get taken in by the bullshit woke propaganda around gender ideology. People who usually ‘follow the science’ seem to turn off that part of their brain and go along with the “be kind, be inclusive” crowd without a second critical thought. Their behaviour boggles the mind.
The information is out there – heck – even in the Calgary Herald. Why are people suddenly so desperately incurious about issues they claim to be staunch and relentless defenders of?
From the Calgary Herald Dr. Roy Eappen Endocrinologist writes –
“As a practising endocrinologist who understands what these invasive and irreversible medical interventions can do to young people, I couldn’t be more supportive of Alberta’s decision to protect children. There’s not nearly enough evidence to justify their use on children, yet there’s plenty of evidence that they harm them.
Unsurprisingly, this move has come under swift attack from some in Canada’s “chattering classes” including journalists, some academics and a few politicians who are either unaware or don’t care about the realities of kids’ bodies.To that end, there has been a torrent of media coverage alleging that Alberta is endangering children and abandoning medicine. That’s false. Sex-reassignment interventions can do serious physical and mental damage, leading to lifelong health programs that would otherwise be avoided.
Besides, Canadians who uncritically support such physical interventions to children and teenage bodies would do well to broaden their horizons. They may be surprised to learn that international organizations and European countries that they commonly look to for leadership are urging the very caution that they oppose.”
Damn, I guess that would make the medical associations in the UK, Sweden, Norway, Finland, Denmark and France ALL SERIOUSLY TRANSPHOBIC.
Along with the hypocrisy the usual woke tactic is to call everything they disagree with as “insert slur here” rather than presenting an argument or compelling evidence.
Dr. Eappen continues:
“Consider the World Health Organization (WHO). Last month, the WHO declined to issue guidelines for transgender procedures for children, on the grounds that “the evidence base . . . is limited and variable regarding the longer-term outcomes.” The words “limited” and “variable” are significant and cautionary. The first, “limited,” means it’s far from clear that so-called “gender-affirming” medical interventions are beneficial. The second, “variable,” hints at the evidence that children who get these interventions suffer. Coming from the World Health Organization, that’s quite a statement indeed.
Or consider Europe. A growing number of countries have already banned or severely restricted children’s access to transgender interventions, based on systematic reviews of the science. That includes England, Sweden, Finland and Norway, while Belgium, France, Ireland and Italy have raised concerns. We’re talking about countries that are generally aligned with Canada, ideologically. They’re looking at the science and seeing red flags. What’s wrong with Alberta doing the same thing?Canadians who reflexively see gender transition as an extension of previous advocacy for gay civil rights should know that it’s not. Instead, “gender-affirming” care for children is essentially gay conversion therapy.Multiple studies have found that most kids who are confused or distressed about their sex end up realizing they’re gay — nearly two-thirds in a 2021 study of boys. Yet if they go down a transgender road, they’ll lose sight of who they really are.
Before England started taking child safeguarding seriously, clinicians at the country’s main transgender service referred to prescribing puberty blockers as “transing the gay away.” They also joked that “there would be no gay people left” if they continued helping kids medically transition. Is that really what Canadians want for our country’s gay and lesbian kids?
The fact is that about 80 per cent of children who believe they’re transgender eventually come to terms with their sex without surgical or pharmaceutical intervention. The worst thing we could do is prevent them from discovering who they really are by pushing them down the road of irreversible medical interventions.
Alberta has joined Saskatchewan and New Brunswick in doing the right thing. Now the rest of Canada should follow suit.”
So it looks like evidence based medicine is transphobic, material reality is transphobic, and really the truth must be at least doubly transphobic.
Link to the Calgary Herald – hhtps://calgaryherald.com/opinion/columnists/opinion-alberta-is-right-children-should-be-protected-from-transgender-procedures
Link to the paper cited – https://link.springer.com/article/10.1007/s11930-023-00358-x
Sorry folks just tired of the fact free hyperbole surrounding the issue. We need to get back to reality based arguments. The sooner the better.
This is exactly the sort of conversations we need to be having here in Canada. The pernicious nature of gender ideology must be exposed and critiqued in the public sphere. People must be allowed to form their opinions based on the facts, not coercion, which is the typical method used when any issue about transgenderism and gender ideology crops up.
Paola Diana is simply on fire in this interview – she dispatches all the tropes thrown at her and women to bully and silence them into submission.



Your opinions…