
You are currently browsing the category archive for the ‘Gender Issues’ category.
The political interests of women are often overlooked by both the right and the left.

The bullshit that goes on because we cannot advance the idea that females are a distinct class of individuals in society who exist solely for themselves. Not in relationship to the family, not in relationship to their reproductive capacity, and most certainly not as an object of desirability for the men-folk. Yet, the old perspectives continue to linger and fester making it difficult for women to fully establish their humanity in society.
The latest assault on female rights and personhood in society has come from “progressive” Left. The notion that because some gender confused males don’t have a uterus, we should erase the terms ‘women’ and ‘females’ in the language of society in a quixotic effort to be more “inclusive”. To explain how erasing women in society is a good thing let’s look at what “Kenny Ethan Jones” has to say –
“Why should we respect and embrace phrases like “people who menstruate”?
When we solely use women to describe people who experience periods, we exclude everyone who doesn’t identify as a woman from the conversation. I’m very familiar with how that exclusion feels and the consequences it can have.
I am a man in [for clarity, ‘Kenny’ is female], I am trans and I sometimes experience periods.
Growing up, periods were my biggest personal struggle. I mean the pain, the bleeding — that sucked. But the most painful part was the internal shame I felt knowing what was happening to my body was something the world only associates with women and girls.
Every scientific study explaining the biology of menstrual cycles, every bit of advertising for period-related products, every piece of language I had ever seen or heard reinforced one thing: boys don’t have periods. I’d known I didn’t feel like a girl long before I ever experienced periods, but I didn’t have any other way of seeing what was happening to my body outside of that one, gendered angle. I felt alienated, isolated. A bodily function that I had no control over caused me to be in conflict with my identity as a man, all because of society’s language and viewpoint on periods.
Although this tweet was very disheartening for me as a trans man, there are plenty of other people who benefit from gender-inclusive language being used when it comes to the period conversation. In fact, linking womanhood so closely with menstruation becomes problematic when you realize how many cisgender women don’t experience periods, and who are no less woman because of it.”
You see? It is the gender religious magic in action. My self declaration should have more importance in society than the medical and biological facts of the matter. It gives me pause when I see an individual so wholly dedicated to a delusional point of view – but on that individual level her views on her gender and her bodily functions are fine. Just like when I see the nice people in white tops and black pants roll up to talk to me about Jebus and Magic Hats, I can politely disagree with what they say and their take on reality, and then they go away (off to find a more receptive victim to lovebomb into their cause).
But tell this gender acolyte to move on with their gender-magic… Well, one should not do that as it qualifies *somehow* as bigotry and hatred on a near cosmic scale. Let’s define bigotry quickly here, just to help frame what is going on.
 I choose not to share in the belief that human beings can change their sex. A man who calls himself a women is still a man. A woman who calls herself a man is still a woman. This two statements though completely true are somehow controversial. Sticking with the version of reality that is closest to the material truth doesn’t seem like bad worldview to hold. I will not participate in gender-magic and really, any ideology that is not moored in the societal reality we all share. And therein lies the rub – gender acolytes won’t accept no for an answer, it is incumbent on *you* to accept *their* version of how sex and gender work.
I choose not to share in the belief that human beings can change their sex. A man who calls himself a women is still a man. A woman who calls herself a man is still a woman. This two statements though completely true are somehow controversial. Sticking with the version of reality that is closest to the material truth doesn’t seem like bad worldview to hold. I will not participate in gender-magic and really, any ideology that is not moored in the societal reality we all share. And therein lies the rub – gender acolytes won’t accept no for an answer, it is incumbent on *you* to accept *their* version of how sex and gender work.
Allow me to say unequivocally, they can fuck right off with their attempted imposition of their beliefs on me. Engage with as much gender-delusion as you please, but keep me out it. At least the formally religious have the good sense to go away once asked they respect the boundaries of others. The gender religious, not so much.
Any ideology or religion that doesn’t respect other’s thoughts and boundaries is dangerous. Gender ideology (GI) is a clear and present danger to women because (GI) seeks to define the term woman (adult human female) out of existence.
Speaking up for women comes with a price. We’ll see if Lord Hunt will be forced to pay it.
 I’d just like to take a small bite of one of the problems that occurs when having discussions with people who believe in the current gender fad. Let’s start with the biggest fish on the plate – what is the definition of being ‘Transgendred’. This from Wikipedia:
I’d just like to take a small bite of one of the problems that occurs when having discussions with people who believe in the current gender fad. Let’s start with the biggest fish on the plate – what is the definition of being ‘Transgendred’. This from Wikipedia:
“Transgender people have a gender identity or gender expression that differs from the sex that they were assigned at birth.[1][2][3] Some transgender people who desire medical assistance to transition from one sex to another identify as transsexual.[4][5]Transgender, often shortened as trans, is also an umbrella term; in addition to including people whose gender identity is the opposite of their assigned sex (trans men and trans women), it may include people who are not exclusively masculine or feminine (people who are non-binary or genderqueer, including bigender, pangender, genderfluid, or agender).[2][6][7] Other definitions of transgender also include people who belong to a third gender, or else conceptualize transgender people as a third gender.[8][9] The term transgender may be defined very broadly to include cross-dressers.[10]
I stopped because I have no idea what a ‘gender identity’ is. So let’s define that.
“Gender identity is the personal sense of one’s own gender.[1] Gender identity can correlate with a person’s assigned sex at birth or can differ from it.[2]Gender expression typically reflects a person’s gender identity, but this is not always the case.[3][4] While a person may express behaviors, attitudes, and appearances consistent with a particular gender role, such expression may not necessarily reflect their gender identity. “All societies have a set of gender categories that can serve as the basis of a person’s self-identity in relation to other members of society.[6] In most societies, there is a basic division between gender attributes assigned to males and females,[7] a gender binary to which most people adhere and which includes expectations of masculinity and femininity in all aspects of sex and gender: biological sex, gender identity, and gender expression.[8] Some people do not identify with some, or all, of the aspects of gender assigned to their biological sex;[9] some of those people are transgender, non-binary, or genderqueer. Some societies have third gender categories.”
The first (of many) problems with these definitions is that they do not correspond to the reality we inhabit:
“Transgender people have a gender identity or gender expression that differs from the sex that they were assigned at birth”
This most basic premise is wrong. Sex is not “assigned” at birth. Sex observed at birth as obstetricians in the vast majority of cases can easily categorize members of the male sex class and members of the female sex class. It is worthwhile at this juncture to note that human beings cannot change the sex that they were born with, simply stated:
Biological sex is immutable.
So we have to note that right from the start, one of the foundational premises of trans-ideology is fundamentally flawed. Any argument based on the premise that sex is assigned at birth will necessarily be false. But, of course, there is just more than one flawed premise in the mix.
“in addition to including people whose gender identity is the opposite of their assigned sex (trans men and trans women), it may include people who are not exclusively masculine or feminine (people who are non-binary or genderqueer, including bigender, pangender, genderfluid, or agender)“
It’s here that swirling morass of haphazard generalizations and faulty reasoning kick in. Gender identity is the ‘personal sense of one’s own gender’. What the hell does that actually mean? What is it like to experience the personal sense of one’s gender?
To be perfectly honest – I have no idea what it is like to experience my own gender. I know what it is like to be me, and my personality, but I have no intuitive sense of what my supposed gender identity is. Try it for yourself describe your ‘gender identity’ to yourself. Try it with this added challenge – describe your gender identity without using sex stereotypes. Here is a handy list you should avoid.

I’ll wait.
…
It would seem like the personal sense of one’s gender identity rests on the adoption of a particular set of negative sex stereotypes about the class of people you happen to be born into. That is what gender is; an arbitrary societally prescribed set of behaviours/expectations that are imposed on females and males in society. These social norms exist in society and are in no way present in human beings prior to social exposure. How do we know this? For instance we know that social gender norms change over time – the girl pink/boy blue situation was reversed or not present prior to the 1950’s. Thus, gender is something that is outside of us and we are exposed to it once we start interacting with society.
So how does one ‘identify’ with being female or male then, without resorting to the (mostly) negative sex stereotypes (a.k.a gender) that society imposes on people? Said another way, what does ‘feeling like’ a man or women feel like?
Sounds like nebulous bullshit to me.
“While a person may express behaviors, attitudes, and appearances consistent with a particular gender role, such expression may not necessarily reflect their gender identity. “All societies have a set of gender categories that can serve as the basis of a person’s self-identity in relation to other members of society.“
We need to approach the idea of ‘identity’ with a great deal of caution because ‘identity’ is inherently subjective and thus unreliable as an indicator of correspondence to reality.
“In most societies, there is a basic division between gender attributes assigned to males and females,[7] a gender binary to which most people adhere and which includes expectations of masculinity and femininity in all aspects of sex and gender: biological sex, gender identity, and gender expression.[8] Some people do not identify with some, or all, of the aspects of gender assigned to their biological sex;“
This sentence conflates the personalities we all have with gender identity and gender stereotypes. You as an individual in society are not a gatekeeper for the gendered expectations that are rightly or wrongly, imposed on you. Most certainly you can defy them, a man wearing pink for instance or a woman being aggressive, but your personal identification is irrelevant to societal expectations. Nor does adopting the stereotypes of the other class of people make you a member of that class of people. A man wearing a dress is still a man.
Should it be okay if a man wants to wear a dress? Absolutely. It should be encouraged as gender non compliant behaviour illustrates the coercive and arbitrary nature of the system we know as ‘gender’.
What wearing a dress for a man does not do is make him a woman.
This is tip of the iceberg level of what is going on in the faux-progressive areas of society. Feelings and the subjectivity inherent within them are being lauded over the empirical reality we all share. The implications for females in our society are quite foreboding, but that is another post.
Gender ideology is totalitarian in nature. There can be no debate, no compromise, and especially no questioning its tenets. Regular everyday people do not realize the poison pill that they swallow when they are told to ‘be kind’ and comply with the reactionary bullshit that is gender ideology. These are some of the questions that you are not supposed to ask, because the answer is almost always ‘because I say so’. So I’ve found a nice chart that will easily identify those that need attitude readjustments so you, my gentle readers, might not be alarmed when faced with this current batch of misogynistic nonsense that has gained so much traction in society.

Oh, and terf is an acronym – Trans Exclusive Radical Feminist – it is a slur like witch, bitch, c*nt et cetera used on uppity females that will not comply with the reactionary bullshit that is gender ideology.


Welcome to the world of male-centric alternative facts. The ACLU have well and truly lost their grip on reality and are inhabiting the same world now as Donald Trump when it come to ‘fake news’ and the willing repetition of falsehood.
Welcome to 2021. :(
The GRA of 2004 gave trans people the ability to change legal sex via a GRC, but only if they had a psychiatric diagnosis of dysphoria and only after having lived in role for 2 years. The spousal veto gave spouses a chance to annul or obtain a favourable divorce.
While this ultimately created the loophole in women’s rights that we’ve been fighting against in the last few years, it catered for a tiny number of dysphoric transsexuals and so did not have an enormous impact.
Discussions with trans friends and allies make it clear that, although surgery wasn’t a requirement for a GRC, the diagnostic procedures were expected to trap and exclude males who did not want surgery, thereby preventing fetishists and opportunists from exploiting a GRC.
The Equality Act of 2010 defined the various protected characteristics, including both sex and ‘gender reassignment’, and provided for sex-based exemptions, under the auspices of which it is legal to exclude trans people from some single-sex spaces and services.
The campaign to reform the GRA to remove medical gatekeeping and make changing gender a matter of self-id was where women put our foot down. The GRA gave a very limited group of MtF transsexuals access to our spaces. Self-id would have made this any man who said he was a woman.
In addition, transactivists were demanding the removal of sex-based exemptions from the Equality Act. This would have left women with no ability to exclude males from any space on any basis, thereby removing every protection gained in the last century of feminism.
This is the effect of self-identified ‘gender identity’ (the ideological concept on which this rides) combined with the deliberate conflation of gender identity with sex. There is no possible point at which women can draw a line.

Our resistance to this campaign was successful; I think most people recognise that it isn’t reasonable to allow any male to identify into women’s spaces on his say-so. It was, however, self-id which was rejected, leaving women’s rights open to further attacks.
Transactivists claim that the current process for obtaining a GRC is invasive and onerous, and continue to push for a reform they claim is ‘merely administrative’ (this doesn’t gel with the attacks on the Eq2010 sex-based exemptions, though: https://t.co/MpxjXv5IoL)
They use the struggles of dysphoric people as a weapon, and by pushing back against self-id we replicate this. Personally I think the best place to attack the ideology is on the conflation of gender identity with sex: https://t.co/zN0ziAZzyM.
If we want fair play for both women and trans women, then it is time to confront the “trans women are women” mantra head-on, highlight why it is misogynistic and deeply harmful to women, and refuse to tolerate its use.
— Caroline – Real Feminists XX \U0001f1ff\U0001f1e6 (@radicalhag) January 16, 2018
This means that we say yes to all the demands of transactivists *except* the one which conflates TW with W, which effectively forces the declaration of a third (and possibly fourth) gender and the provision of facilities for them.
It means we’re onboard with self-id, access to medical care, non-discrimination, ability to serve in the military etc, which of course we should be in any case. We do NOT want to get gaslit into a kneejerk rejection of anything trans, which makes us sound like rightwingers.
BUT it also means we insist on a positive, sex-based definition of woman, and force TRAs to show their hand. We know perfectly well what we’re dealing with here; we want to force them to demonstrate to the public that their agenda is access to women’s spaces, not trans rights.

This worked like a bomb when the UK govt provided a trans prison wing so they could remove MtFs from the female estate. The squawking and wailing about being ‘othered’ and ‘caged’ was epic, and Joe Public went “Yeah, right.”
Basically it’s a position which says: you’re free to have a gender identity. You’re not free to tell me *I* have a gender identity. And you are definitely not free to tell me that your gender identity is in any way comparable to my sex.
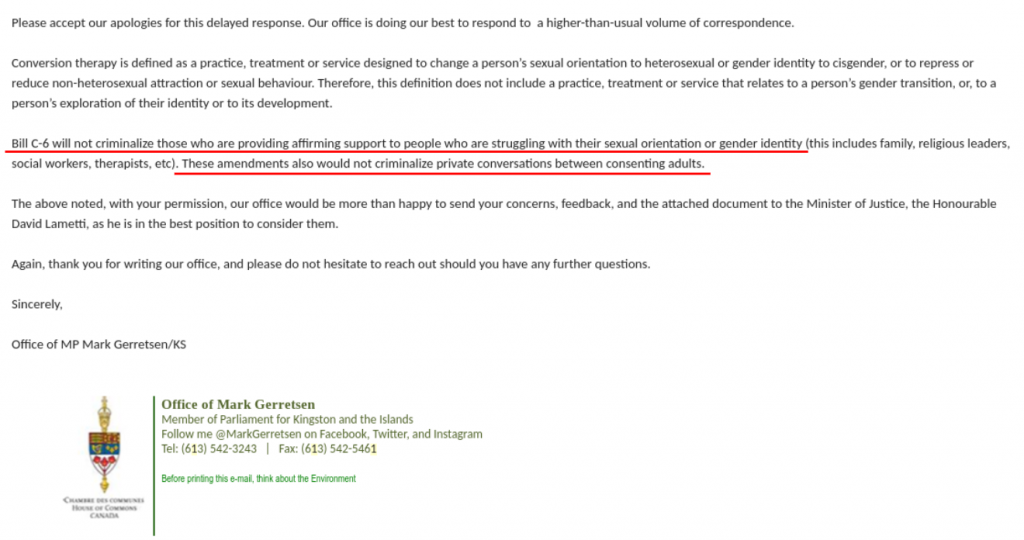
Contact your MP and get them to stop this bill. Pronto. (Text from the Canadian Gender Report)
“Liberal MP Mark Gerretsen has confirmed in an email to one of our members that Canada is about to impose criminal penalties for parents, therapists and other healthcare professionals who do not offer “affirming support” to children who are experiencing gender dysphoria. The proposed Bill C6 will amend Canada’s federal criminal code that purports to ban conversion therapy. As we can read from the admission of MP Gerretsen, Members of Parliament do not understand the implications of “affirmation” with respect to the type of support offered to youth struggling with their gender identity. The effect of Bill C6 will impose the narrow and poorly understood medical transition pathway recently coined “gender-affirming care”.
What is “affirming”?
The usage of the word “affirming” to qualify the type of support that can be provided to children and youth is very deliberate and needs to be explained as distinct from other clinical approaches.
Affirmation is a new treatment approach to children and adolescents experiencing gender dysphoria. The “affirming care” protocol dictates that medical interventions such as puberty blockers, cross-sex hormones and irreversible surgeries be provided to youth based on their self-directed gender “goals”.
The previously established clinical protocol of watchful waiting provided a supportive approach whereby children can be gently questioned about why they’ve started to identify as a different gender so that parents, clinicians and others can develop a complete picture of the child’s needs and keep all options open to help the child resolve feelings of gender dysphoria without pushing them towards irreversible medical interventions. This more cautious model of care has been phased out in favour of “affirmation” at Canadian gender clinics.
The affirming model of care is an extremely risky approach because it does not allow a healthcare professional to explore how underlying factors may be contributing to a young person’s newly adopted gender identity and feelings of gender dysphoria. Issues such as childhood trauma, psychiatric symptoms such as cutting or self-harm behaviours, autism or ADHD, feelings of shame due to same-sex attraction and many other issues a young person may be struggling with are often entangled with symptoms of gender dysphoria.
An “affirming” approach to care hides these other issues and does not allow for the possibility that other factors may be the cause of a young person’s new-found gender identity and be driving the need to medically transition as a coping mechanism.
The distinction between the previous, more cautious model of care and the new “affirmation” model is that children could be supported in their gender exploration without the need for all adults to agree and “affirm” that, in reality, the child actually “is” the opposite sex or a gender of their choice and provide them with whatever medical means they desire to transform their bodies to match their gender identity.
Gender activists promote affirmation and social transition because this is viewed as supportive to transgender adults who have transitioned. “Affirming support” is designed exclusively for the needs of this group, not the needs of young people who are struggling to find appropriate care for their complex and individual needs and where social and medical transition may not be appropriate for their long-term well being.
From “Affirming Support” to Puberty Blockers and More
The assessment process in place in Canadian gender clinics has become more and more narrow in scope over the past few years. The requirement for any type of mental health assessment has been removed completely in over 50% of the gender clinics in Canada. The only purpose of the remaining assessment process is to validate whether youth meet very minimal criteria to proceed with hormones and seem to be capable enough to sign a consent form.
In fact, we were shocked that SickKids considered the long wait time to access an initial appointment at their gender clinic as an advantage as children would have this time for “considering options”. This is an admission that the assessment process at Canada’s largest gender clinic is not intended to determine who may be a good candidate for medical transition, but in fact, all children with a gender identity that does not match their biological sex are considered candidates for medical transition and it is only their “goals” and ability of the child to “reflect on their gender journey” that might determine otherwise.
“Affirming support” as a treatment protocol removes safeguarding and impacts informed consent
Gender-affirming care is a narrow treatment pathway that does not allow the clinician to explore other options with young people as a means for managing their gender dysphoria. Today, youth are being referred to pediatric endocrinology clinics by their GP’s while it’s unclear to both the patients and the referring physicians that these clinics have adopted a pro-medical transition policy whereby the onus of responsibility is placed on the child or adolescent to guide the assessment process. In many cases we are aware of, it is up to the young person to refuse invasive hormonal interventions when these are offered as the treatment pathway by the presumably “expert” staff at the gender clinic.
Consider, for example, these scenarios that erode proper safeguarding for youth who are considering medical gender transition:
It is not considered “affirming” to help young people find mental health support for managing their gender dysphoria as an alternative to medical gender transitioning. We have heard several scenarios of young adolescents expressing doubt over transitioning to their healthcare team, including telling them that they are experiencing anxiety and/or depression. As a matter of course, young people are being told that these symptoms will subside once they start their prescriptions of Lupron or testosterone and are not being offered any further help to understand the root cause of their anxiety, depression or other factors they later realize have led them to believe they needed to transition.
It is not considered “affirming” to be honest with young people considering medical gender transtition that many adolescents become comfortable in their own bodies and re-identify with their natal sex given time, and that some adults express regret at having transitioned. This information is not considered “affirming” of the group of people who have transitioned and are living as a different gender because it casts doubt at whether their lived experiences as the opposite sex has permanence and validity.
“Affirmation” has become an ideologically driven philosophy of care that effectively removes safeguards including the ability for youth to be informed of the risks and consequences of medical transition necessary to be able to consent to these experimental interventions.
Further evidence that medical gender transitioning of children in Canada has become a matter of personal autonomy can be found in this policy document of CPATH, the Canadian arm of the World Professional Association of Transgender Health, which clearly advocates for a ban on “gender conversion therapy” (Bill C6) in order to ensure that transgender people do not face any barriers to medical transition services. CPATH does not consider the age of the person making the decision to transition as relevant.
This position presumes a “one-size-fits-all” affirmation and transition approach for children and adolescents which ignores the experience of desistors, a majority of cases where young people become comfortable in their natal sex.
Why has the treatment protocol changed?
It’s unclear why the treatment protocol has evolved to an “affirmation” approach rather than a more cautious clinical approach although the WPATH organization that sets the standard of care has gone through a significant change in leadership and approach over the past decade and has become advocates for transitioners rather than an objective organization that is free from conflicts of interest.
The affirmation model (treatment with puberty blockers followed by cross-sex hormones and gender-affirming surgeries) comes from the Dutch Protocol developed to support children with early-onset childhood dysphoria who did not desist from intense and persistent feelings of gender dysphoria with the onset of puberty. One of the key authors of that model has issued a warning in Pediatrics that it was never intended for the new population of adolescents that are being unquestioningly “affirmed”. Dr Annelou DeVries acknowledges the phenomenon of ROGD (recent-onset gender dysphoria with no documented history in early childhood) which was not a part of the previous studies on hormone blockers.
Finland and Sweden have conducted systematic reviews of gender treatment of children and both came to the conclusion that there was insufficient evidence for an affirmative approach. Finland developed their own clinical guidelines for treating children which includes significant caution compared with the “affirming” approach in place in Canadian gender clinics.
The UK now requires a best-interest court order prior to any youth being referred to a gender clinic. This has become the strictest requirement in the world to ensure that children are not being medically transitioned if there isn’t clear evidence that it’s in their best interests. The UK National Health Service is also conducting a review of the medical treatment protocol for transgender youth. This was prompted by detransitioner Kiera Bell’s second lawsuit which challenged the MOU on Conversion Therapy, a document similar to Bill C6, because she was unquestioningly affirmed as a boy and was irreversibly harmed by this approach.
Do Children Have the Capacity to Consent?
The underlying assumption of gender affirming care is that children and youth are capable of informed consent to an experimental pathway of medical treatments. Kiera Bell challenged this assumption in a judicial review last year and won her case. A key factor in the landmark decision by the UK High Court in December 2020 which now requires a “best-interest court order” to be in place prior to children being referred to gender clinics is that the clinics themselves do not understand the risks or benefits of hormone interventions including puberty blockers and cross-sex hormones on children and youth, therefore it is not likely that children are capable of consenting to medical interventions that will have such life-changing effects.
Conclusion:
It is already extremely difficult for parents, trans-identified youth and detransitioners to access non-invasive and agenda-free healthcare options in order for them to receive a differential diagnosis prior to medical transitioning or to receive support to manage symptoms of gender dysphoria without being medicalized.
We are asking for the following exemption to be added to Bill C6 to ensure healthcare professionals are able to support youth effectively:
For greater certainty, this definition does not apply to any advice or therapy provided by a social worker, psychologist, psychiatrist, therapist, medical practitioner, nurse practitioner or other health care professional as to the timing or appropriateness of social or medical transition to another gender, including discussion of the risks and benefits and offering alternative or additional diagnoses or courses of treatment.
Without this exemption, Bill C6 will further entrench the doctrine of “affirmation” in the Canadian healthcare system. While all individuals should be treated with dignity and respect, the poorly understood approach of gender-affirming care is being challenged around the world for leading children down a narrow treatment pathway of invasive and often irreversible medical interventions. Our government should be protecting the interests of all youth by conducting an independent review of gender transition services including a review and evaluation of whether children possess the ability to consent to the life-altering treatments that are being offered to them under the mantra of “affirming”.


Your opinions…